 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
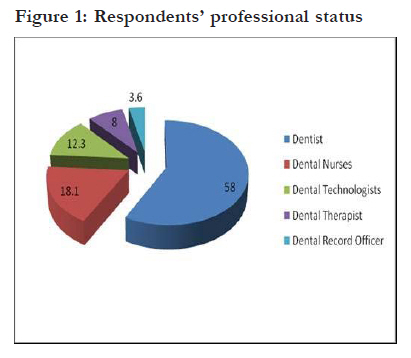
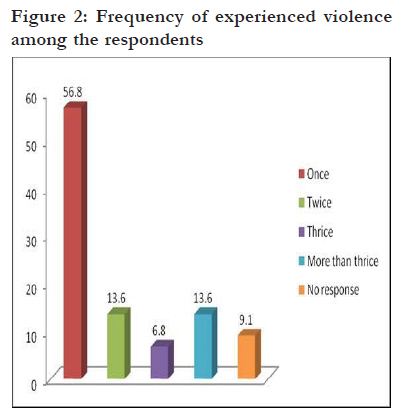
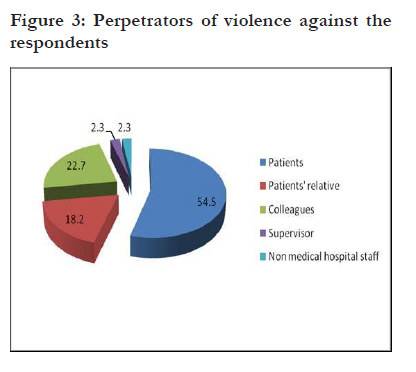
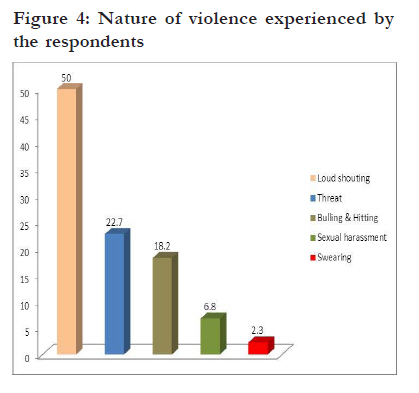
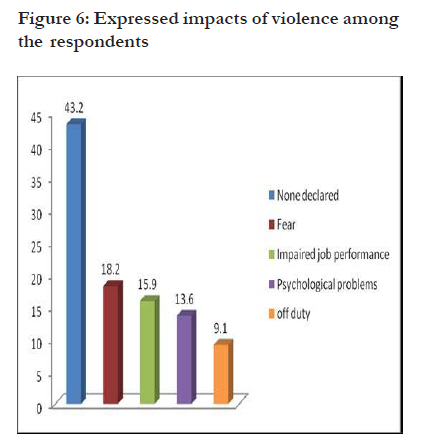
African Health Sciences, Vol. 11, No. 3, Sept, 2011, pp. 486 - 492 Occupational violence against dental professionals in southern Nigeria *Azodo CC1, Ezeja EB2, Ehikhamenor EE3 1 Department of Periodontics, University of Benin Teaching Hospital, Benin City, Nigeria, 2 Department of Preventive Dentistry, University of Benin Teaching Hospital, Benin City, Nigeria, 3 Department of Restorative Dentistry, University of Benin Teaching Hospital/Save Accident, Victim of Nigeria (SAVAN) Code Number: hs11097 Abstract Objective: To determine the prevalence of workplace violence in Oral healthcare centres against Nigerian dental professionals. Keywords: Occupational violence, oral healthcare, dentist, dental auxiliaries Introduction Violence in the workplace is a multi-faceted, multicausal, public health, social and legal problem facing all occupations worldwide1-6. It is considered to be a reflection of the level and wave of violence suffered in the whole society. Violence is an everyday reality for many workers, substantiating the prevalence as an epidemic in all continents of the world7-8. Violence is the third leading cause of death in the workplace9 and also accounts for 16% of more than 1 6.5 million acts of violence experienced by individuals age 12 and over10. The quantification of economic costs of work place violence showed that almost two million workdays and millions of dollars are lost annually because of non-fatal assaults suffered at the work place11. Violence at the workplace is a serious safety and health issue as it increases anxiety and undermines the health worker’s ability to focus on the delivery of safe, effective and competent care12. Many healthcare workers will experience work place violence at least once during their professional career. Nearly a quarter of the world’s work place violence occurs in the health sector and this has led the Australian Institute of Criminology to certify the health sector as the most violent industry in 1999. World Health Organization, International Council of Nurses and Public Services International have also recognized workplace violence as a major health priority13. In America, Centers of Disease Control and Prevention has declared violence in the workplace, a national epidemic because of the pervasive nature14. The impact of violence at work has widespread consequences. It not only affect the employees but also the work places, colleagues, employers, families and society as a whole. It exhibits a dramatic impact on the health, safety and welfare of workers15. It has a substantial effect on staff wellbeing and job satisfaction15,16. Physicians have reported that violence experienced at the work place had a negative impact on their family and on their quality of life17. Work related violence also hampers work performance and causes employee attrition18. It causes low morale and decreased worker productivity which in turn results in monetary loss for businesses and the worker1,19,20. Violent incident at a work place leading to anger, humiliation, shame, frustration, fearfulness, stress, flashbacks, sleeplessness, burnout, lack of motivation, loss of confidence, reduced self-esteem, anxiety, depression, irritability, increased job stress, poor job performance, lower commitment to work, increased sickness absence, post-traumatic stress disorder, psychological disorders, tobacco, alcohol and drug abuse18,20-28. It may even culminate in occupational accidents, invalidity and suicide. Violence come from outside as well as from inside the workplace and ranges from threats and verbal abuse to physical assaults and homicide but Health care employees are more likely to experience verbal abuse12. In the health sector, the perpetrators are mainly patients and their relatives12. Others include supervisor, hierarchical superiors, fellow-workers, subordinates or even complete strangers29,30. Violence gainst health workers is found in all areas of practice and constitutes a serious hazard. A variety of factors make health workers particularly prone to the acts of violence and they include; working with people under the influence of drugs or alcohol, mentally ill people, unrestricted movement of the public in clinics and hospitals, the increasing presence of gang members, long waits in emergency or clinic areas that lead to client frustration over an inability to obtain needed services promptly and lack of staff training and policies for preventing and managing escalating hostile and assaultive behavior3,17,28,31-35. Aggression management training has been shown to result in fewer incidents, less serious incidents, a reduction in the psychological sequalae following incidents, improved response to incidents and better staff morale36. Numerous studies on occupational violence have been conducted for medical doctors17,37-42, nurses24,25,28, mental health staffs43,44 and emergency department staffs45-48 but there are only a few studies for dental professionals49. To the best knowledge of the researchers, there is no information on occupational violence in Nigerian oral healthcare centres in published literature. The objective of this study was to determine the prevalence of workplace violence in Oral healthcare centres against Nigerian dental professionals. Methods A questionnaire-based cross-sectional survey of 175 randomly selected dental professionals working in Oral healthcare centres of University Teaching hospitals in Southern Nigeria was conducted in 2009. The hospitals were University College Hospital, Ibadan; University of Benin Teaching Hospital, Benin City; Lagos University Teaching Hospital, Idi-Araba and Obafemi Awolowo University, Ile-Ife. All these five Teaching Hospitals are actively involved in undergraduate and postgraduate training of dental workforce and have all cadres of dental professionals in their employment. The sampling technique employed was systematic sampling. In each of the study locations, a list of dental professionals present at work was obtained. Every third person on the list was selected until a total of 35 in each were selected. Dental professionals that were on leave or absent at work for any reason on the day of the study were excluded. The questionnaire elicited information on demography, prevalence of violence in the last 12 months, types, perpetrators, reasons and expressed impacts of the violence. Informed consent was obtained prior to the onset of the survey, the survey was anonymous and participation was voluntary. Ethical approval for this study was obtained from University of Benin Teaching Hospital Ethics committee. Data analysis was done using Statistical Package for Social Sciences (SPSS version 15.0). The test for significance was done using chi square statistics and a p < 0.05 was considered significant. Results The survey response rate was 78.9%. The respondents were dentists (58%), dental nurses (18.1%), dental technologists (12.3%), dental therapists (8.0%) and dental record officers (3.6%) as shown in [Figure - 1]. The prevalence of violence in Nigerian Oral healthcare centres was 31.9%. More than half of the dentists and dental auxiliaries in this survey experienced violence only once in the last 12 months as indicated in [Figure - 2]. There was no statistically significant difference in the prevalence of violence against dentist and dental auxiliaries. The main perpetrators of the violence were patients (54.5%) and patient’s relatives/friends (18.2%) as indicated in [Figure - 3] below. Non-physical violence in form of loud shouting (50.0%) threat (22.7%), sexual harassment (6.8%) and swearing (2.3%) constituted the majority while physical violence in form of bullying and hitting constituted the remaining 18.2% as shown in [Figure - 4]. Violence was often associated with long waiting time (27.3%), cancellation of appointment (13.6%), outcome of patient’s treatment (11.4%),alcohol intoxication (9.1%), psychiatric patient (6.8%), patient’s bill (4.5%) and others (27.3%) as shown in [Figure - 5]. The expressed impact of violence among the respondents include fear 8 (18.2%), impaired job performance 7 (15.9%), psychological problems 6 (13.6%) and off duty 4 (9.1%). No impact was declared by 19 (43.2%) as shown in [Figure - 6]. Discussion The economic downturn, poverty, rising unemployment and easy firearm accessibility have made the society, more violent and dangerous than ever before. There exists mounting evidence to suggest that workplace violence towards healthcare professionals is a common and widespread problem. Disturbance in the social fabric of the society accounts for increasing levels of violence in the work place. In this study, the prevalence of violence in Nigerian Oral healthcare centres was 31.9% which is lower than the 38% violent incidents recorded among public health field workers50, 49.5% recorded among health workers in Turkish health care settings51 and 63.7% documented among general practitioners working in urban areas of New South Wales, Australian38. This is higher than the 21% documented among general practitioners in Dublin, Ireland52, 24.3% documented among health-care workers in an Obstetrics and Gynaecology unit of a Nigerian University Teaching Hospitals53 and 24.6% documented among health workers in their first year of employment54. Frequent contact of oral healthcare workers with people in distress and pain may be responsible for the level of violence reported in this survey. Widespread poverty and inequality may also have eroded friendly disposition of patients and their relatives thereby manifesting with violence against oral healthcare professionals in Nigeria. Studies have shown that females are more common victims of violence in the health care setting38, 49,51,55. In this survey, there is no significant difference in the prevalence between males and females. Occupational violence is not acceptable, no matter how frequently or infrequently it occurs. In this study, 56.8% had experienced violence only once within the last 12 months. The workplace in general has traditionally been viewed as a relatively benign and violence-free environment. In hospitals, health care workers believe their mission is healing and are usually caught unaware by violence during the discharge of their duty or anywhere in the workplace. Patients and their relatives or friends are most common perpetrators of workplace violence in health sector3, 4, 12,27,28,32,33,51,56 . In this study, the main perpetrators of the violence were patients (54.5%) and patient’s relatives/friends (18.2%). Uneven distribution of oral health centres, manpower shortages and the increasing level of oral diseases among the Nigerian populace result in crowding in waiting room. Long waiting time accounted 27.3% of violence in this survey. Violence in the health sector has been associated with long the waiting time in previous studies35,57. In emergency departments in Denizli, Turkey, the second most frequent reason for violence was long waiting times34. Cancellation of appointments occurs when the optimal working environment for successful delivery of oral health services is hampered. It is usually associated with distress and may manifested by violence because a patient would have sacrificed the day’s work in order to receive dental treatment. In this study, cancellation of appointments was responsible for 13.6% of the reported violence. The mouth functions in mastication, deglutition speech and also contributes to facial aesthetics and psychological well being of an individual. An error in from dental treatment adversely affects social interaction, quality of life and facial aesthetics. It is therefore not surprising that the outcome of treatment emerged as the third single most common reason for violence in this study. Studies revealed that dissatisfaction with treatment and failure to meet patients’ expectations are among chief causes of violence in health care settings3,17. Research studies consistently find that alcohol use is associated with verbal and physical violence in the work place58. Increasing drug and alcohol use have also been implicated in the rise in violence59. In this survey, alcohol intoxication accounted for 9.1% of the violence. Mental illness contributes to violence against healthcare workers. Several oral conditions manifesting in mentally ill patients making them frequent recipients of oral care. In this survey, psychiatric patient were responsible for 6.8% of the reported violence. Furthermore cost of treatment was the reason for 4.5% of the violence in this survey. Deprivation, poverty and unemployment and lack of health insurance are common among people seeking dental care in Nigeria. It is assumed that perception of the cost of care as being expensive will trigger a violent reaction from patients and relatives. Health care workers are at risk of both fatal and non-fatal violence-related injuries. Violence may also consist of repeated actions which, by themselves may be relatively minor, but which can cumulatively come to constitute serious forms of violence such as sexual harassment, bullying or mobbing. Verbal abuse has long being recognized as the most prevalent form of violence in workplace worldwide5,12.15,16,34,35,38,46. In this study, the nonphysical violence form constituted the majority. Workplace violence is one of the most complex and dangerous occupational hazards facing people working in a healthcare environment. Violence at work not only has an immediate effect on the victim, but also expands in progressively larger ripples, affecting other people directly or indirectly, as well as the enterprise and the community28. In this survey, no impact was declared by 43.2% of the respondents, while expressed impacts include fear (18.2%), impaired job performance (15.9%), psychological problems (13.6%) and being off duty (9.1%). An urban inner-city tertiary care centre survey in Vancouver showed that about three quarters of emergency departments staff that have experienced violence were afraid of patients as a result of violence and almost half hid their identities from patients16. A study on health care workers in emergency departments in Denizli, Turkey also revealed that 36.1% of workplace violence victims developed psychological problems after the incident34. Variability in the impact of violence could be due to the fact that victims respond differently to violence and also the support received may be contributory. Conclusion The prevalence of workplace violence in Oral healthcare centres against dental professionals in Southern Nigeria was significant and had a substantial effect on dental professionals’ well-being thus necessitating urgent attention. Improved patient care efficiency and communication may clarify expectations and prevent frustration and angry verbal outbursts. These data would also serve as valuable data for health care managers and policy makers in planning violence reduction intervention. References
African Health Sciences Vol 11 No 3 September 2011 The following images related to this document are available:Photo images[hs11097f5.jpg] [hs11097f4.jpg] [hs11097f3.jpg] [hs11097f2.jpg] [hs11097f1.jpg] [hs11097f6.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}