 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
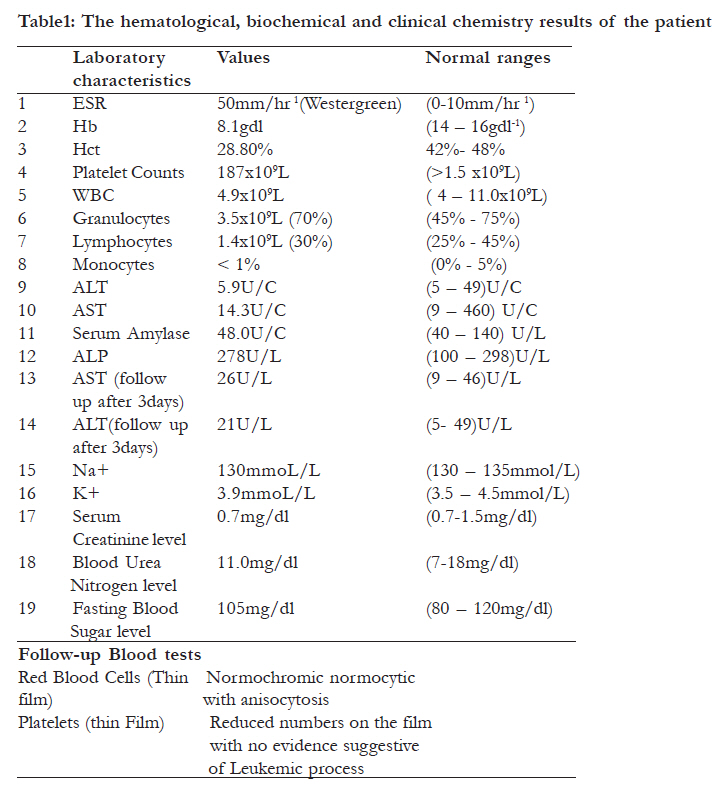
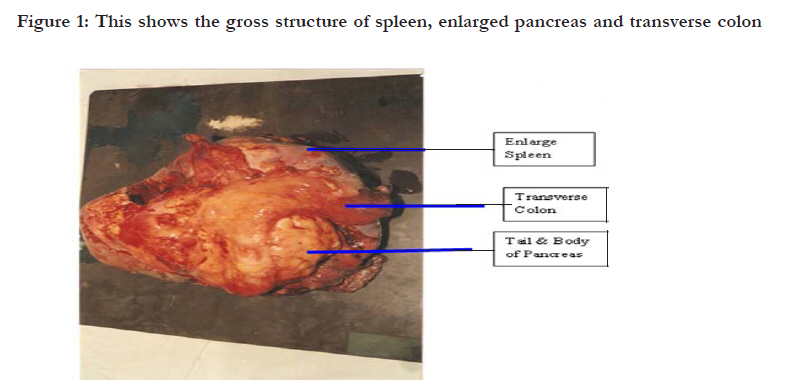
African Health Sciences, Vol. 11, No. 3, Sept, 2011, pp. 449 - 453 Pancreatic cancer in an 18-year-old boy Kitara DL1 , Wabinga HR2 1 Department of Surgery, Faculty of Medicine, Gulu University, Gulu, Uganda, 2 Department of Pathology, College of Health Sciences, Makerere University, Kampala, Uganda Code Number: hs11099 Abstract We report a case of histopathologically proven pancreatic cancer in an 18-year-old boy. Complete blood picture revealed moderate normochromic normocytic anaemia with anisocytosis. Other laboratory results including liver function tests, renal functions tests, serum amylase, fasting blood sugar level and serum electrolytes were all of normal values. Abdominal US showed a focal mass of the pancreatic body and tail with involvement of the spleen and the transverse colon. Laparotomy confirmed the sonographic findings and demonstrated adhesions of the transverse colon to the mass at the splenic hilum. Histology of the mass showed a well differentiated adenocarcinona of the body and tail of the pancreas. This highlights the differentiation of pancreatic cancer from autoimmune pancreatitis and, to a lesser extent, other forms of pancreatitis and benign pancreatic lesions. Key words: Pancreatic cancer, laparotomy, distal pancreatectomy, ultrasonography. Introduction Pancreatic cancers are rarely present in childhood and present a markedly different prognosis than adults1,2. Diagnostic difficulties and inappropriate treatment may occur due to variable clinical appearanc illness1. A 26 year audit (19681984) at the Polish-American Institute of Pediatrics, faculty of Medicine, Jae of thegiellonian University, Krakow, Poland showed 5 patients ranging in age from 5-14 years who were operated upon for pancreatic tumours, four of which were malignant2. We present an 18 year old school boy who was successfully managed surgically at Mulago National Referral Hospital, Kampala, Uganda. Case report An 18-year-old boy presented to Mulago outpatients department with a history of progressive abdominal swelling and dull aching abdominal pain mainly at the epigastrium. The abdominal pain was radiating to the back and only partially relieved by analgesics. These previously mentioned symptoms were not associated with vomiting, constipation, yellow eyes, loss of appetite or weight loss. The patient denied any history of smoking and there were no previous similar episodes or relevant family, medical or surgical history. On general examination, he had normal vital signs apart from signs of anemia; he was afebrile and was not jaundiced. There was epigastric tenderness with firm, nodular mass not fixed to the posterior abdominal wall. The spleen was massively enlarged and nodular. There was no renal or suprapubic tenderness. The rectum was full of fecal material with normal anal tone. Complete blood picture revealed moderate normochromic normocytic anemia with anisocytosis. Other laboratory results including liver function tests (ALT, AST, and serum protein levels); renal functions tests (serum creatinine, blood urea and nitrogen levels), serum amylase, fasting blood sugar level and serum electrolytes (K+, Na+) were all within normal range. Abdominal US showed an enlarged pancreatic body and tail with involvement of the spleen and the transverse colon with no abnormalities of the other abdominal organs. The patient was successfully managed surgically in Mulago National Referral Hospital. He underwent laparotomy revealing gross splenomegaly, with multiple firm nodular masses, which were arising from the body and tail of the pancreas. There were adhesions of the transverse colon to the mass at the splenic hilum. There was no gross evidence of lymphatic or local spread to the retroperitoneal spaces. The liver surface was smooth with no gross evidence of any metastatic sites. Splenectomy was performed, resection (>10cm long) and primary anastomosis of the transverse colon with silk 2/0, distal pancreatectomy (body &tail) and pancreatic discharged after 10 days. He continued his follow duct was transfixed with silk No.1. A sump drain up in the surgical outpatient department (SOPD) and was instituted at the pancreatic bed and the abdomen cancer institute for adjuvant chemotherapy. In the was closed in layers. The sump drain was removed subsequent review in the SOPD two weeks later, 48 hours after surgery. The abdominal stitches were the patient was reexamined and was investigated for removed in 14 days and the wound had healed liver enzymes, pancreatic enzymes, renal function completely. Histology showed a well differentiated tests, serum electrolytes, chest x-ray and complete adenocarcinoma of the pancreas. The patient did blood picture which all were within normal range. very well in the post-operative period and was discharged after 10 days. He continued his follow up in the surgical outpatient department (SOPD) and cancer institute for adjuvant chemotherapy. In the subsequent review in the SOPD two weeks later, the patient was reexamined and was investigated for liver enzymes, pancreatic enzymes, renal function tests, serum electrolytes, chest x-ray and complete blood picture which all were within normal range. [Table - 1], [Figure - 1] and [Figure - 2] Discussion The true incidence of pancreatic cancer (PC) is not well known in Uganda. A review of the Kampala Cancer Registry in the Department of pathology in Mulago National Referral Hospital showed that over a period of 5 years (1999 to 2003), there were only two cases of pancreatic cancers reported in those below 30 years (Kampala Cancer Registry – unpublished data). Risk factors for PC include: age > 603, male sex (likeliness of up to 30% over females)3, African-American ethnicity, cigarette smoking4 Diets low in vegetables and fruits, diets high in red meat, diets high in sugar-sweetened drinks, obesity, Diabetes mellitus3,14 and chronic Pancreatitis has also been linked15. The risk of PC in individuals with familial pancreatitis is particularly high and in individuals with Helicobacter pylori infection. Five to ten percent of PC patients have a family history of pancreatic cancer 8. It has been associated with the following syndromes; autosomal recessive ataxiatelangiectasia and autosomal dominantly inherited mutations in the BRCA2 gene and PALB2 gene, Peutz-Jeghers syndrome, Lynch syndrome, familial adenomatous polyposis, and the familial atypical multiple mole melanoma-pancreatic cancer syndrome (FAMMM-PC)3,8,Gingivitis or periodontal disease. None of these were observed in this patient. The possible differentials in this patient could have been Autoimmune Pancreatitis (AIP) and other rare lesions of the pancreas5. The AIP in younger patients has distinct clinical features, such as presentation with epigastralgia, back pain without jaundice, and elevated serum amylase levels5. Autoimmune pancreatitis is a chronic inflammatory condition with distinct clinical, radiographic, and histologic features6. On ultrasonography for AIP, the involved pancreatic parenchyma appears hypoechoic, consistent with edema6. The US finding in AIP is different from that of pancreatic carcinoma5,6. Typically, AIP will have imaging that reveals a “sausage-like” pancreas with delayed enhancement on CT scan, rim enhancement on T2 weighted MRI, or hypoechoic pancreas with echogenic spots on ultrasound5. AIP rarely causes calcification or pancreatic pseudocyst, but can cause localized enlargement which can contribute to the difficulty in differentiating it from PC malignancy5, 6. Imaging studies, such as computed tomography (CT scan) and ultrasound (US) can be used to identify the location and form of the pancreatic cancer7. Because MRI and CT scans were not available at this resource limited hospital, Ultrasound was used for making diagnosis for this patient. The pathological features of lymphoplasmacytic infiltration and fibrosis are often used as the gold standard for the diagnosis of autoimmune Pancreatitis9,10. In addition to lymphocytes, the inflammatory infiltrates in autoimmune pancreatitis may contain macrophages, mast cells, neutrophils, and eosinophils. Nonnecrotizing granulomas are occasionally seen, including periductal granulomas10. The histologic diagnosis can be made in patients who have any or all of the following three most common histologic features of autoimmune pancreatitis11,1 Conclusion Patients diagnosed with pancreatic cancer typically have a poor prognosis partly because the cancer usually causes no symptoms early on, leading to locally advanced or metastatic disease at the time of diagnosis. Median survival from diagnosis is around 3 to 6 months, 5-year survival is less than 5%9, and PC may occasionally result in diabetes. Insulin production is hampered and it has been suggested that the cancer can also prompt the onset of diabetes and vice versa14. Thus diabetes is both a risk factor for pancreatic cancer and diabetes can be an early sign of the disease in the elderly. The findings in this young man were different and eight years later, the patient is still alive and well. Acknowledgement I acknowledge with appreciation the participation and support of the late Dr. WW Obote for the encouragement he gave to the surgical team to enable us successfully manage this patient in Mulago Hospital, Kampala, Uganda. References
African Health Sciences Vol 11 No 3 September 2011 The following images related to this document are available:Photo images[hs11099t1.jpg] [hs11099f2.jpg] [hs11099f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}