 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
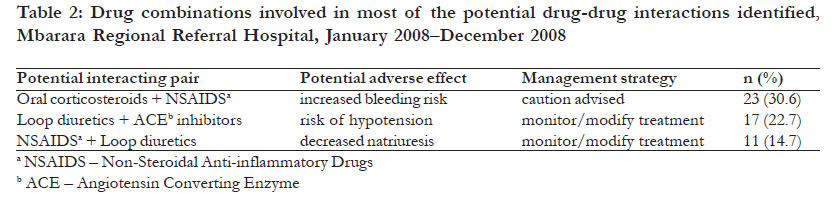
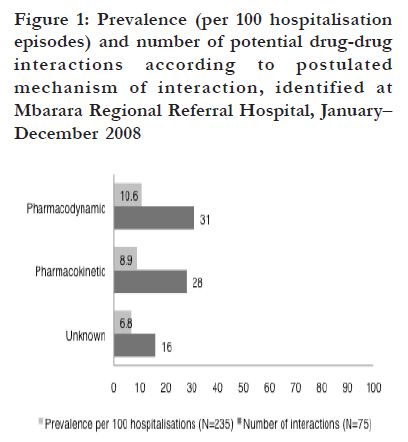
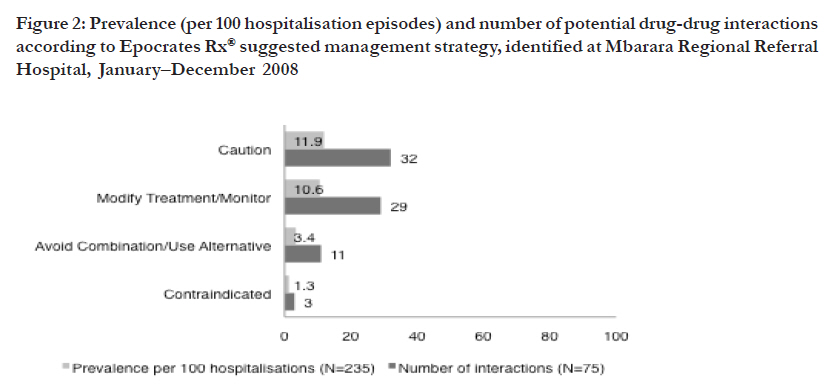
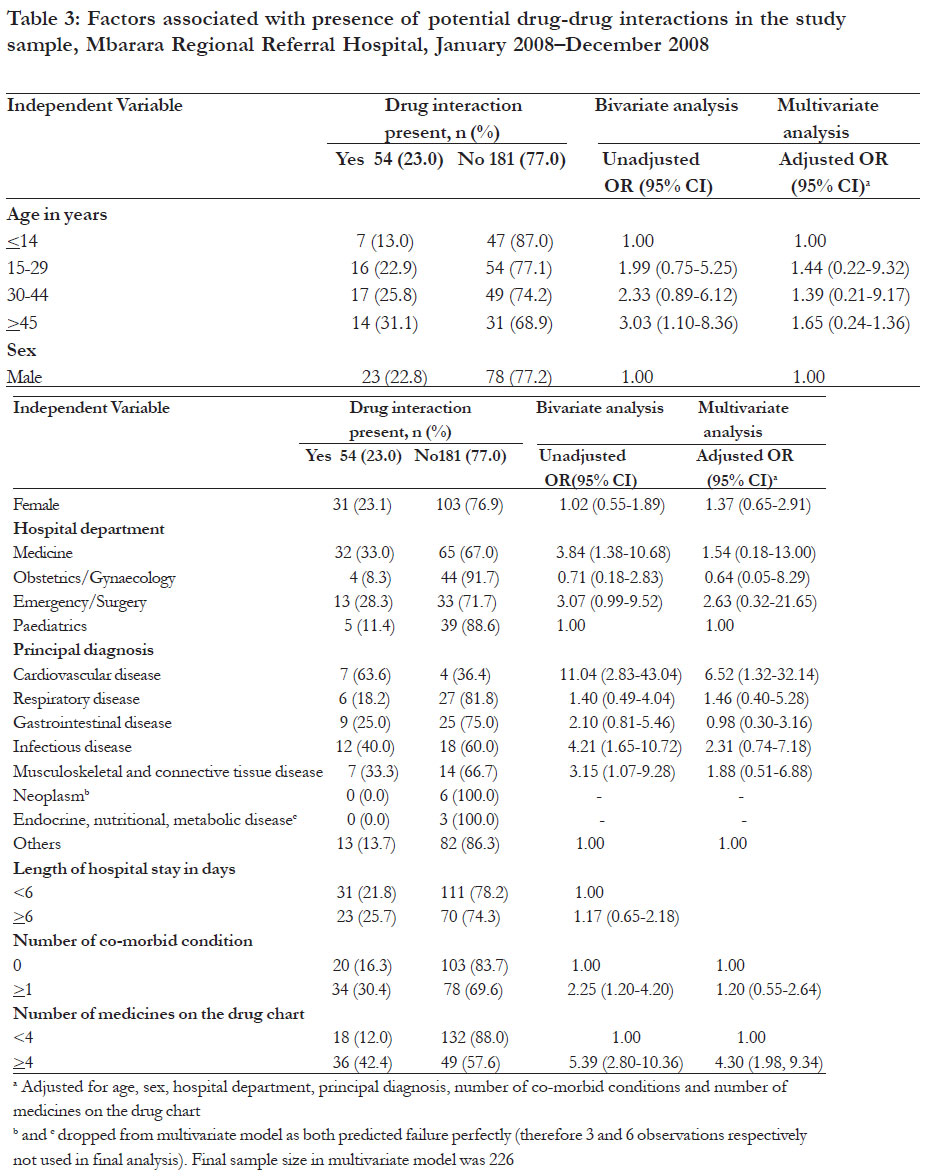
African Health Sciences, Vol. 11, No. 3, Sept, 2011, pp. 499 - 507 Potential drug-drug interactions on in-patient medication prescriptions at Mbarara Regional Referral Hospital (MRRH) in western Uganda: prevalence, clinical importance and associated factors Lubinga SJ*, Uwiduhaye E Department of Pharmacy, Mbarara University of Science and Technology, Mbarara, Uganda Code Number: hs11100 Abstract Background: Drug-drug interactions (DDIs) are an important cause of adverse drug reactions. The pharmacoepidemiology of such interactions in hospitals in Uganda is not known. Key words: drug-drug interactions, pharmacoepidemiology, prevalence, chart review Introduction Drug-drug interactions (DDIs) occur when the effects of a drug are changed by the presence of another drug, resulting in synergistic, additive or antagonistic outcomes and are an important cause of preventable adverse drug events1. Pharmacoepidemiologic studies, mostly carried out in Europe and the Americas, have found varying rates of potential DDIs, ranging from 5 to 80%2-6, owing to variations in methodology and differences in definitions of potential DDIs. DDIs have been shown to lead to increased hospitalization, increased length of hospital stay, morbidity7-9, mortality10, and increased financial costs8, 9. Factors that have shown consistent association with the presence of potential DDIs in previous studies included polypharmacotherapy, age, gender, main diagnosis and medication and the number of physicians a patient visits2, 5, 9, 11, 12 . However, studies documenting potential DDIs in sub-Saharan Africa are fewer. In Kenya about 33.5% of patients receiving antiretroviral medications were exposed to clinically significant drug interactions with their antiretroviral medications13. To our knowledge, no previous study has attempted to document the pharmacoepidemiology of potential DDIs among general in-patients in Uganda. In this study, we determine the prevalence and clinical importance of, and factors associated with potential DDIs at a referral hospital in western Uganda. Methods Sample and settings We conducted a retrospective analysis of hospitalization episodes (medication charts and medical notes) from the four major departments: medical, surgical, obstetrics/gynaecology and paediatrics wards of Mbarara Regional Referral Hospital (MRRH), a 240 bed-hospital in Western Uganda, with an approximate annual enrolment of 17,400 patients. We reviewed charts and notes over a 12-month period from 1st January 2008 to 31st December 2008. Medication charts and accompanying notes were included if at least two medications had been prescribed. We excluded charts and notes for which background information was incomplete. Our final sample size was 228. We adopted a stratified random proportionate sampling strategy. All hospitalization episodes within the study period were stratified according to hospital department and the study sample drawn randomly in a ratio of 2:1:1:1 (Medical to Obstetrics/ Gynaecology to Surgical to Paediatrics), reflecting the relative admission numbers for each department. Procedures For each medication chart, the data collected included generic and/or trade name of medications, dosage regimen, start date and stop date. We extracted background information from the corresponding medical notes, including age and sex, principal diagnosis and co-morbid conditions based on the International Classification of Diseases, 10th revision (ICD-10) codes, and the length of hospital stay computed as the number of days from admission to discharge. Analysis of potential DDIs Potential DDIs were identified using Epocrates Rx® online premium, a freely available online medical decision support tool that provides current and clinically relevant information concerning drug interactions. It screens for potential DDIs and classifies them according to mechanism as pharmacokinetic, pharmacodynamic or unknown and by management strategy as contra-indicated (life threatening and permanent damage may be induced, they should not be co-administered); avoid combination/ use alternative (can cause therapeutic problems/ difficulties but may be administered together if the patient is carefully monitored); modify treatment/monitor (cause increased or reduced effects but to a lesser extent, effects are mainly expressed in already chronic disease compromised patients) and caution (caution on use, mainly cause unimportant effects and no specific action is required). According to Perkins et al14, Epocrates Rx® has perfect sensitivity scores (1.0) and a specificity of 0.9 in detecting clinically significant DDIs. Dallenbach et al15 also found that it had a sensitivity of 81% (95%CI 77-85%) and a specificity of 88% (95%CI 86-89%) when compared to the opinion of a clinical pharmacologist using drug-drug interaction compendia. We opted to use this software because it was freely available, regularly updated and only needed an Internet connection to analyse the interactions. Drugs were considered for potential DDI analysis if their dosage schedules overlapped for at least 24 hours. Data analysis Our unit of analysis was a single hospitalization episode. Descriptive analysis was conducted for background characteristics. We computed the total number and prevalence of potential DDI, defined as number of medication charts with at least one potential DDI per 100 hospitalization episodes, as well as number and prevalence of potential DDIs specific to potential DDI mechanism and suggested management strategy. To determine the factors associated with potential DDIs, we conducted a bivariate analysis with “presence of potential DDI” as the dependent variable and the following independent variables: age, gender, principal diagnosis, length of hospital stay, presence of at least one co-morbid condition, number of medicines on the medication chart and hospital department. Explanatory variables with a p value of 0.1 or less as well as the person-level variables: age, sex and hospital department were then entered into a multivariate logistic regression model to determine factors independently associated with the presence of potential DDIs. The model was evaluated using a block entry procedure. Analyses were conducted using STATA 10 (Stata Corporation, TX, USA) and graphs were drawn using Microsoft® Excel 2008 for Mac. Ethical issues Ethics approval was obtained from the Faculty of Medicine Research and Ethics Committee of Mbarara University of Science and Technology. The drug and therapeutics committee of Mbarara Regional Referral Hospital was informed that the study was being carried out and ethical approval had been obtained. Results Background characteristics Two hundred thirty five hospitalization episodes were analyzed for potential DDIs. The median (IQR) age was 30 (0-85) years. One hundred thirty four (57.0%) were women. Ninety-seven (41.3%) were from the general medical department, 47 (20%) from the obstetrics/gynaecology, 51 (21.7%) from emergency/surgery and 40 (17%) from the paediatric department. The median (IQR) length of hospital stay was 5 (3-7) days. The median (IQR) number of medicines on the drug charts was 4 (3-5), and 85 (36.2%) charts had four or more medicines. One hundred and eleven (47%) of the charts were for patients with at least one co-morbid condition [Table - 1]. Potential DDIs A total of 75 potential DDIs were identified in our study. Fifty-four medication charts had at least one potential DDI out of 235 hospitalization episodes giving an overall prevalence of approximately 23 per 100 hospitalization episodes. Fourty-one (17.4%) charts had 1 potential DDI, 8 (3.4%) had 2 potential DDIs, 2 (3.9%) charts had 3 and 3 (1.3%) charts had 4 potential DDIs. Interactions were most prevalent in the medical department (n=32; 33%) followed by the emergency/surgery (n=13; 28.3%), paediatrics (n=5; 11.4%) and obstetrics/gynaecology (n=4; 8.3%) departments. The majority of potential DDIs were postulated to occur through a pharmacodynamic mechanism (n=31, prevalence=10.6%) followed by pharmacokinetic (n=28, prevalence=8.9%). The mechanism was unknown for 16 interactions (prevalence=6.8%) [Figure - 1]. With regard to clinical importance, most (n=32, prevalence=11.9%) interactions required “use with caution” as a management strategy. Twenty-nine (prevalence=10.6%) were “modify treatment/monitor”, 11 (prevalence=3.4%) were “avoid combination/use alternative”, while 3 (prevalence=1.3%) were “contraindicated” combinations [Figure - 2]. The two contraindicated combinations were diclofenac and aspirin (n=1) and rifampicin and fluconazole (n=2). Three potential DDIs accounted for over 60% of the interactions identified: corticosteroids and NSAIDS (30.6%), diuretics and ACE inhibitors (22.7%) and NSAIDS and antihypertensives (14.7%), see [Table - 2]. Factors associated with potential DDIs In bivariate analyses, several factors were associated with the presence of a potential DDI including increasing age in years, hospital department, a principal diagnosis of cardiovascular disease, infectious disease, or musculoskeletal/connective tissue disease, having at least 1 of co-morbid condition, and 4 or more medicines on medication chart [Table - 3]. After adjusting for potential confounders and person level variables, two factors, a principal diagnosis of cardiovascular disease (versus others, OR 6.52 95% CI 1.32-32.14) and 4 or more medicines on the medication chart (OR 4.30 95% CI 1.98-9.34) were independently associated with the presence of a potential DDI [Table - 3]. Discussion Prevalence of potential DDIs In our sample of 235 medication charts, we found a prevalence of potential DDIs of 23 per 100 hospitalisation episodes. This is a relatively high figure that highlights the importance of this previously unstudied problem in Uganda. Although our methodology and definitions might have differed from those used in other studies, the results fall with in the range cited previously (5-80%). Studies that have looked at prevalence of interactions among hospitalized patients have yielded similar results. In Brazil, Moura et al9 have shown that 37% (n=589) of patients in a general hospital were exposed to one potential DDI while Cruciol-Souza and Thomson12 found a frequency of potential DDIs identified using the DrugReax® system of 49.7% in a teaching hospital. Vonbach et al6 found that 56.2% (n=851) of the patients in a Swiss hospital were exposed to at least one potential DDI of major or moderate severity as defined by Pharmavista®, a drug interaction program. Potential DDIs were most prevalent on the general medical ward. The prevalent conditions on this ward, for example cardiovascular diseases and infectious diseases particularly HIV/AIDS and opportunistic infections lend themselves to use of more complex drug regimens with a higher potential for interactions. General medical patients also have a higher number of co-morbid conditions and take more medicines than those from other departments. These patients therefore need closer monitoring to avoid the potential negative outcomes of DDIs. Clinical importance of potential DDIs We used the suggested management strategy as a surrogate measure of severity/clinical importance of the interactions identified because we did not have access to the commercial computerized drug interaction software that provide information on severity of drug interactions and levels of evidence supporting the presence of drug interactions. Nonetheless, like with other studies4, 6, 12, clinically important potential DDIs were rare. Only 3.4% and 1.3% of hospitalization episodes having interactions classified as “avoid combination/use alternative” and “contraindicated” respectively. In our study, we found that one patient had been prescribed aspirin at 300mg three times daily together with Diclofenac at 50 mg three times daily. The use of aspirin at higher doses of >325mg/day with other NSAIDs is contraindicated. When co-administered, protein binding of diclofenac is reduced resulting in higher concentrations of free diclofenac in the blood. Although the clinical significance of this interaction is unknown, co-administration is generally not advised because the combination may increase the risk of NSAID adverse events such as gastrointestinal bleeding and renal toxicity. Rifampicin is a known potent inducer of the cytochrome p-450 enzyme system. Panomvana Na Ayudhya et al16 have shown that, when administered at different doses among Thai HIV patients, rifampicin significantly altered the pharmacokinetics of fluconazole resulting in a 39% increase in elimination rate constant, 28% shorter elimination half-life, 22% decrease in area under the concentration-time curve, 17% decrease in maximum concentration and 30% increase in clearance. Although co-administration reduced fluconazole blood levels to below the Minimum Inhibitory Concentration for Cryptococcus neoformans, the clinical significance of this interaction is still unknown16. Patients still receive this combination when they suffer from both tuberculosis and cryptococcal meningitis. In such cases, increasing the dose of fluconazole may be considered and these patients should be monitored long term for recurrence of cryptococcal meningitis. Drugs combinations commonly involved in potential DDIs In our study, the most common potential DDI involved the concurrent use of NSAIDS with the systemic corticosteroids, prednisolone, and hydrocortisone, which has been associated with increased risk of gastrointestinal toxicity, including inflammation, bleeding, ulceration, and perforation. Piper et al17 have shown that elderly patients who used corticosteroids and NSAIDs concurrently had a risk for peptic ulcer disease that was 15 times greater than that of nonusers of either drug. Mechanistically, the ulcerogenic potential of NSAIDS coadministered with systemic steroids may be related to the NSAID induced inhibition of prostaglandin production, an increase in neutrophil activation, and gastric hypermotility, and alteration of normal epithelial renewal by the steroid18. When used together, caution is advised, especially in patients with a prior history of peptic ulcer disease or gastrointestinal bleeding and in elderly and debilitated patients. During concomitant therapy, patients should be advised to take the medications with food and to immediately report signs and symptoms of gastrointestinal ulceration and bleeding such as severe abdominal pain, dizziness, lightheadedness, and the appearance of black, tarry stools. In patients who have had previous gastrointestinal ulceration, prophylactic anti-ulcer therapy using the prostaglandin E1 analogue, misoprostol should be considered. The second most common interaction identified in our sample was between both loop and thiazide diuretics and ACE inhibitors. The exact mechanism of this interaction is unknown, however, inhibition of conversion of angiotensin I to angiotensin II by ACE inhibitors lowers aldosterone levels and subsequently leads to sodium and water depletion19. Clinically, in patients who have been sodium and/or volume depleted by the thiazide or loop diuretics, initiation of ACE inhibitors can produce a severe, albeit transient postural hypotention19. It is worth noting that hypotension is not a contraindication to ACE inhibition, in fact, this combination is often exploited for its clinical advantages in both hypertension and congestive heart failure. In patients who need the combination, ACE inhibitor may be initiated at a low dose titrating upwards to the target dose20. Underlying volume depletion may be corrected prior to initiation of ACE inhibitor by either discontinuation or reduction of the dose of the diuretic or prior increased salt intake20. If hypotension occurs, the patient can be placed in a supine position. If it persists, patients can be rechallenged at half the previous dosage, and if on a diuretic, the dosage should be reduced or held for three days before reattempting therapy20. The potential interaction between NSAIDS and loop diuretics also emerged as important in our study. NSAIDS have been shown to antagonize the antihypertensive effects of several antihypertensive drugs including the loop diuretics21, 22. Specifically, NSAIDS particularly indomethacin and ibuprofen, decrease the natriuretic effect of loop diuretics with a resultant decreased antihypertensive effect or decreased diuresis23, 24. This interaction, modulated by NSAID induced renal prostaglandin inhibition, was most pronounced in patients on sodiumrestricted diets24, which is typical of the advice given to patients with hypertension and heart failure. Therefore when used together, patients should be monitored carefully, and where necessary, diuretic dosage increased or the anti-inflammatory agent changed. Factors associated with the presence of a potential DDI A principal diagnosis of a cardiovascular disease independently increased the odds of having one or more potential DDIs almost 7-fold. This is consistent with previous studies in family medicine clinics in Mexico2, and a Brazilian Teaching Hospital12 that showed increased odds of potential DDIs among cardiology patients. This is not surprising as drugs prescribed for cardiovascular diseases including diuretics, ACE inhibitors, B-blockers, and aspirin and statins for primary and secondary prevention of sequelae (e.g., coronary artery disease, myocardial infarction, stroke) are often used in combination and as described above contributed the majority of interactions in our study. We have also shown that patients receiving 4 or more medicines are at an increased risk of potential DDIs. Polypharmacotherapy has been shown in previous studies to be associated with potential DDIs2, 3, 9, 11, 12, 25. Patients receiving medications for cardiovascular diseases and those with 4 or more medicines therefore should have their prescriptions vetted more carefully and be monitored more closely by clinicians and pharmacists. Study limitations The principal limitations of this study are the retrospective design and use of medical records and prescription medication histories as data sources. Causal associations were therefore difficult to infer, and we could not ascertain with any accuracy the completeness or reliability of the information obtained. As such, it is possible that we could have under- or over reported the potential DDIs. Some drugs were prescribed as required and although every attempt was made to match the dosage schedules with the record of medicines administered, we could not accurately determine whether these drugs were actually taken with others, making assessment of an interaction difficult. We could only assess potential DDIs as we were unable to tell from medical notes, conclusively whether a DDI had occurred or the consequences of the interaction. Lack of electronic medical record systems and prescription databases meant we were able to assess only a small sample size, limited to one year’s data. Our findings may also not be generalisable outside the settings of Mbarara Regional Referral Hospital. Conclusion We have demonstrated that a freely available on-line medicine information tool, Epocrates Rx®, can be used to study the pharmacoepidemiology of potential DDIs. Such a tool may be useful in routine clinical practice in the detection and management of potential DDIs. There are freely available versions of this tool for most smart phones and Personal Digital Assistants that can be freely updated over a wireless Internet connection. These may be made available to clinicians at the hospital to support clinical decision-making. Potential DDIs occur frequently in MRRH although clinically significant interactions are rare. Continuing education of prescribers and use of electronic decision support tools may help abate the problem, and follow up may be needed to ascertain the clinical consequences of important interactions. Patients with cardiovascular diseases and those who are prescribed multiple medications need to be monitored more closely as these are at a higher risk of potential DDIs. Acknowledgements The authors would like to thank the records’ officers at Mbarara Regional Referral Hospital for their help in identifying and organizing the charts and medical records. We thank Mr. Norbert Anyama of the Department of Pharmacy, Makerere University College of Health Sciences for his help in reviewing our manuscript. We received no funding for this study. References
African Health Sciences Vol 11 No 3 September 2011 The following images related to this document are available:Photo images[hs11100t3.jpg] [hs11100t2.jpg] [hs11100f2.jpg] [hs11100t1.jpg] [hs11100f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}