 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 11, No. 3, Sept, 2011, pp. 508 - 517 Nutrition Social determinants of breastfeeding in Italy *Kambale M J Independent researcher, Via Leopardi,12/A, 60015 Falconara M (Italy)
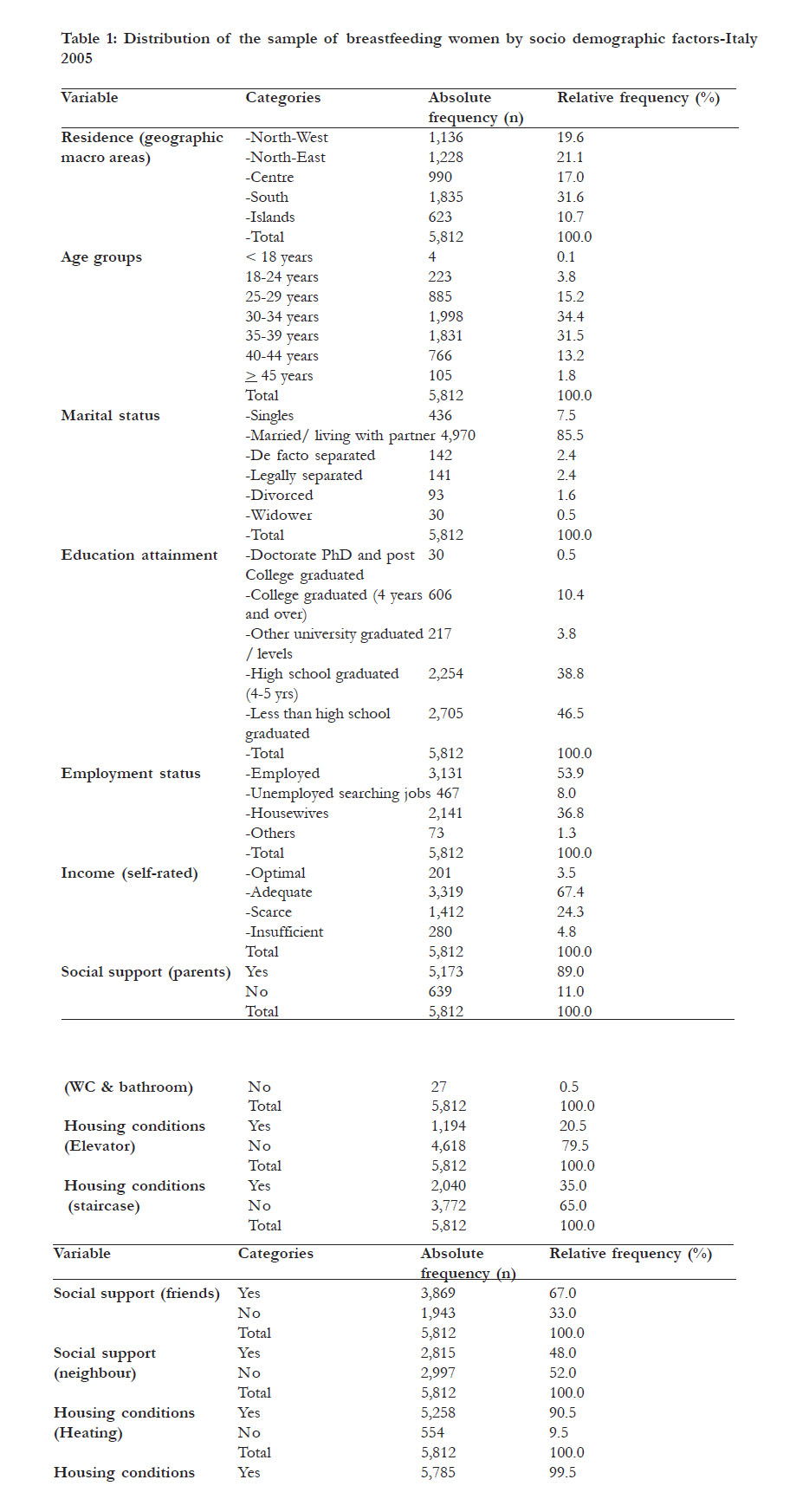
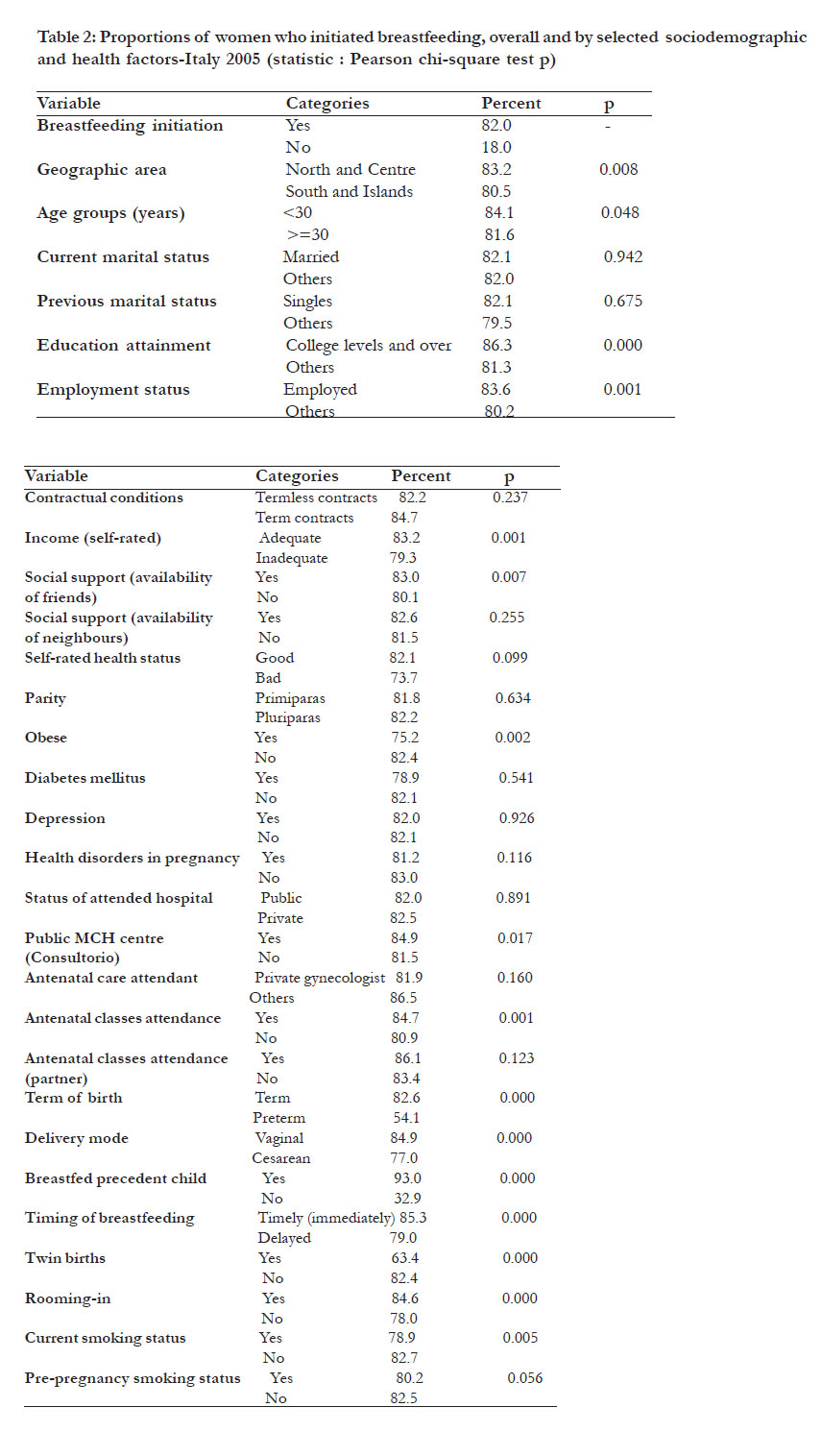
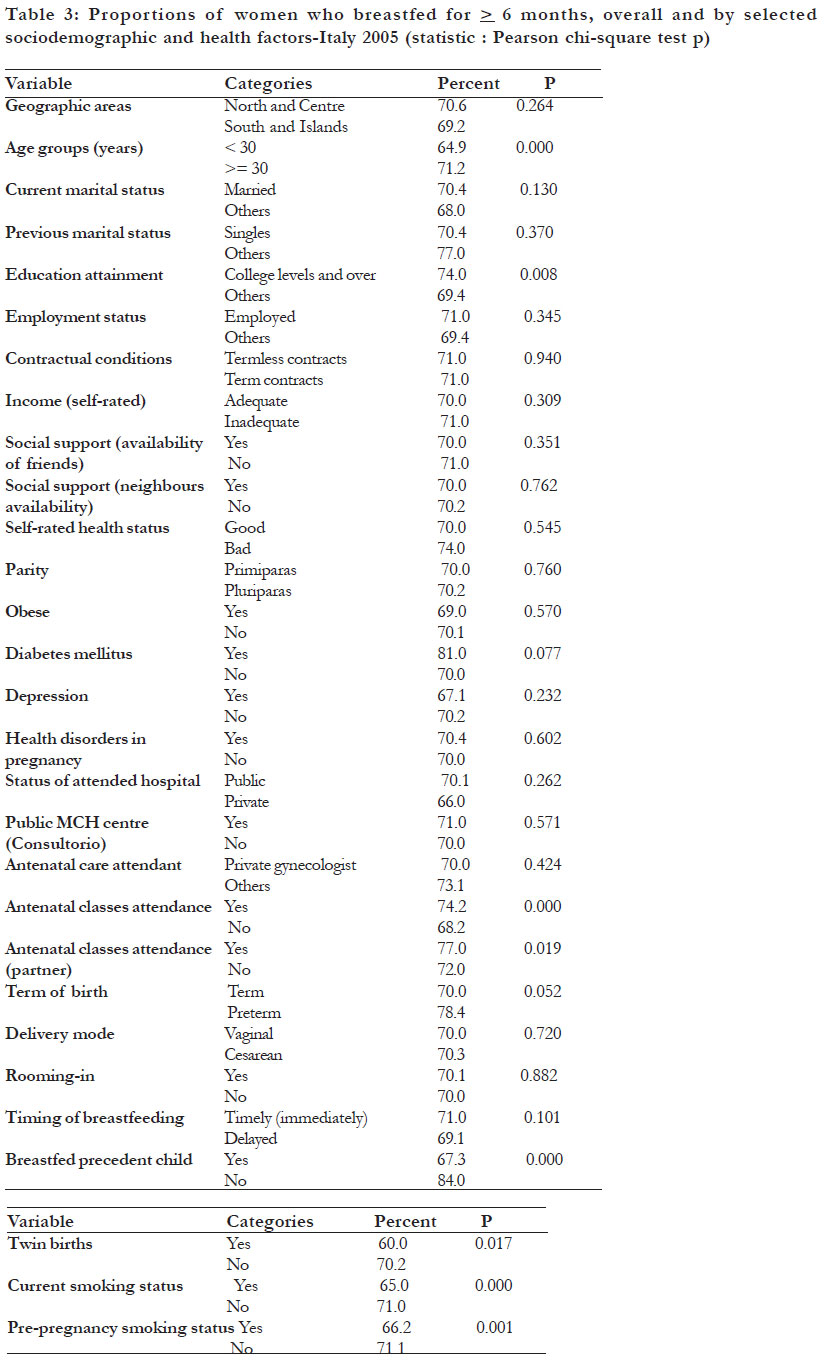
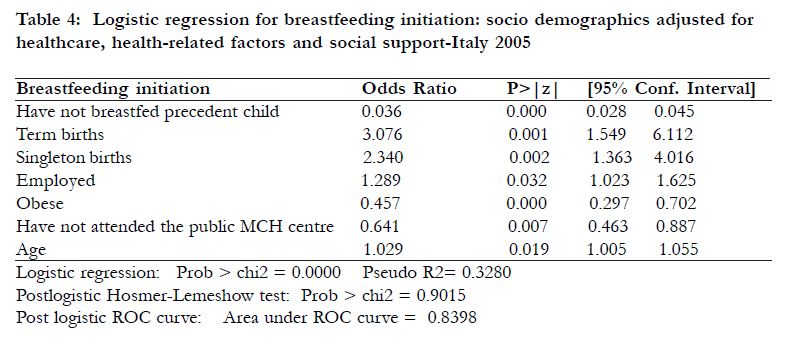
Code Number: hs11101 Abstract Background: Breastfeeding is surely the best way to feed an infant at least in the first six months of life. Keywords: Socioeconomic factors, epidemiologic factors, breastfeeding, Italy. Introduction Exclusive breastfeeding is the healthiest way to feed an infant in the first six months of life1. According to an American Academy of Paediatrics policy statement, “breastfeeding ensures the best possible health as well as the best developmental and psychosocial outcomes for the infant”2. However, many child bearing women don’t breastfeed. Data from several studies suggest that women of lower socioeconomic status (SES) are less likely to breastfeed their infants3-5. Maternal education attainment has been largely investigated in relation to breastfeeding initiation. Results constantly showed a positive association3,6-10. Income is another factor largely studied. It may be that because maternal income is associated with employment, it may detract from breastfeeding11-13. Maternal employment has been shown in some studies to decrease breastfeeding14-16. As pointed out above, maternal employment may be an obstacle because of time taken away from the baby (11-13); in fact some studies found that full-time, but not part-time, employment was negatively associated with breastfeeding initiation17,18. The characteristics of the workplace seem also to have an impact on breastfeeding behaviour. In fact, a study by Jacknowitz, in USA, showed that the availability of employer-sponsored childcare services increased the likelihood of breastfeeding six months after birth by 47 percent19. In addition, working an additional eight hours at home per week, at the mean, increased the probability of breastfeeding initiation by eight percent and breastfeeding six months after birth by 16.8 percent19. Other factors like single marital status8,20, lack of support11,21,22, low parity4,23,24, preterm births5,25,26, obesity 23,25,27 maternal , smoking/ alcohol consumption9,11,23,28-30, diabetes mellitus26 and maternal distress have also been shown to be strongly associated with lower rates of breastfeeding initiation. Ethnic minority groups are frequently recorded as having high rates of positive breastfeeding practices but there are as always some exceptions 7,8,12,31,32. Duration of breastfeeding is also important for the health of the newborn and has been shown to be associated with diverse socioeconomic factors1, 11, 21,33,34. This study intended to investigate the social factors associated with breast feeding initiation and duration in Italy during the period 2000-2005 and thus update the current literature on the subject. Methods Design and tool Data for this study were drawn from the Italian national institute of statistics (ISTAT) survey conducted in 200535. This is a quinquenal multi purpose population-based cross-sectional survey with a complex design (stratified multistage random sampling). The 2005 survey comprised a nationally representative sample of 50,474 households (128,040 subjects). However the immigrants group was not mentioned in the survey. The survey excluded residents of rest homes, religious houses, penitentiaries and homeless subjects. This 2005 ISTAT survey asked several questions to women who delivered (n=5,812) in the past five years prior to the survey about their breastfeeding behaviours including whether (yes vs. no) the mother ever breastfed her infant (breastfeeding initiation) and if the action was on-going. Duration of breastfeeding was assessed asking the women “what age in months and weeks had the baby when he stopped suckling?” The comprehensive questionnaire used in the survey (filled and administered by ISTAT professionals) included socio demographics, health, healthcare and health-related factors. Variables As dependent variables, we used breastfeeding initiation (as defined above) rate and breastfeeding duration rate for e” six months respectively while explanatory variables consisted of all relevant available sociodemographics (age, marital status, education attainment, employment status, contractual conditions, income, etc…), health factors, healthcare and health-related behaviours and finally social support defined as availability of friends and/or neighbours aids in situations of need (yes vs. no). Demographics and socioeconomic status were assessed by using age, residence (5 categories: North-West, North-East, Centre, South, Islands), housing conditions (availability of WC and bathroom, heating and staircase), education attainment (college levels vs. others), occupation status (employed vs. others), contractual conditions (term vs. termless contracts) and self-reported wealth using income as a proxy (optimal-adequate vs. scarce-inadequate). Statistical analysis Virtually all the variables were systematically dichotomized by appropriate procedures in order to perform univariate tests (T-Student test, Pearson chi-squared test). Multiple logistic regressions included binary and dummy variables but age was consistently treated as a continuous variable. We first performed descriptive statistics, then followed with student t-test and chi-squared test in order to examine relationships between several variables and breastfeeding initiation/duration rates. We finally conducted multiple logistic regressions. Models included sociodemographic factors adjusted for potential confounders (healthcare, health and health-related factors and social support). Models’ fitting was based on stepwise backward selection strategy while the diagnosis was conducted by recourse to the standard post logistic tests (Pseudo-R2, post logistic Hosmer-Lemeshow test and ROC curve). Levels of statistical significance were set to 0.05. Odds ratio with 95 percent confidence intervals were calculated to assess the adjusted risk of independent variables and those with p<0.05 were retained in the final models. Analyses were carried out by the statistical package 10.1/SE (36). Results Sociodemographics Our sample comprised 5,812 women (respondent women who delivered the past five years prior to the survey). South macro area shared the highest proportion (31.6 percent; n=1,835) of this sample while the Islands had the lowest (10.7 percent; n=623 (Tab.1). Mean age of this population was 34 years (Standard deviation SD: 5.22) with a minimum of 17 and a maximum of 49. The bulk of this population group was concentrated in the age groups 4 (30-34 years; 34.40 percent) and 5 (35-39 years; 31.5 percent), 85.5 percent were married or living with the partner, 14.7 percent were university/college graduated or had some college education, 54 percent is actually employed and eight percent were unemployed searching job and finally only 3.5 percent rated their income as being optimal [Table - 1]. Breastfeeding behaviours Of these 5,812 respondent women, 18 percent (n=1,044) never breastfed the index child, 82 percent (n=4,168) had done so at least once and 10.3 percent (n=599) were still breastfeeding. The North/Centre and South/the islands are areas which recorded respectively the highest (83.2 percent) and the lowest (80.5 percent) rates of breastfeeding initiation. Similar differentials were also found among several other social and health/health-related factors [Table - 2]. Geographic location (p=0.008), age (p=0.048), education attainment (p=0.000), employment status (p=0.001), income (p=0.001), and social support/ availability of friends (p=0.007) were the sole social factors significant in univariate analysis [Table - 2]. Women who breastfed for six months or more were 70 percent (n=4,070); distribution of breastfeeding duration by specific factors is not presented in [Table - 3]. Detailed results of multivariate analyses are presented in [Table - 4] (only breastfeeding initiation). Older ages (OR:1.029, 95CI: 1.005-1.055; p=0.019) and employment status (OR: 1.289, 95CI: 1.023- 1.625; p=0.032) are the only social factors associated with breastfeeding initiation while no significant social determinant of breastfeeding duration was found. Finally, reasons for not breastfeeding (not displayed in tables!) included lack of milk (63.4 percent), newborn’s difficulties in sucking milk (14 percent), maternal health problems (10 percent), new-born health problems (six percent) and social problems like lack of time and employment constraints (three percent). Discussion Overall, 82 percent (n= 4,768) of the women from this sample had breastfed their infants at least once. This is substantially similar to values reported in studies conducted in many other countries worldwide and higher more than some others3,7,12,37,41. Precedent population-based studies conducted in Italy, also using nationally representative samples, showed breastfeeding initiation rates of 89 percent (n=3,500) in 1999 in Banderali’s study and 85.3 percent (n=1,601) in Giovannini’s. The latter had evidenced significant geographic differentials with rates ranging from 75.8 percent in the islands to 90.8 percent in North-east area42,43. In our study, the highest scores were also recorded in the North-East geographic area (86.4 percent) and among age the group 25-29 years (84.4 percent) while the lowest were found in the Islands (76.1 percent) and among the age group > 44 years (74.3 percent). This geographic differential, also reported in the study of Giovannini, is consistent with the well-known socioeconomic differential North-South in health already documented in Italy43,44. Another Italian study conducted in Liguria region in 2003, however of a different design (a cohort hospital-based study) and a more limited scale (n=757), showed rates of breastfeeding initiation of up to 97.3 percent at discharge34. As showed in a precedent paragraph, the proportion of women who breastfed for six months or more after childbirth were 70 percent [Table - 4], this is a very satisfactory score if compared to the 19 percent at six months reported in a precedent Italian study43. We found a significant positive association between breastfeeding initiation, age, education attainment, high income and social support, a result consistent with international literature3,5-9,21,31,45. In fact elders, highly educated and wealthy women are usually expected to have better breastfeeding behaviours. Our study did not find (adjusted model) an association between breastfeeding initiation and marital status despite the fact that this association is widely reported in literature8,11,14. The fact also that we found a positive association between employment status and breastfeeding initiation is in odd. In fact, employed women are frequently recorded as having lower likelihood of breastfeeding11-14. Bias in data collection or management is improbable but can’t be ruled out. For example the response rate of this survey was not specified, a defect with potential impact on the results. If this rate was low, it might have had a significant negative effect on the representativeness of the study. Likewise the exclusion of the immigrants, currently an important sociodemographic group of Italian society with high birthrate, is a serious issue. Other alternative explanations include the fact that employed women usually are the most educated and so are probably more sensible with breastfeeding promotion programs or perhaps most of these working women were part-time employees, a factor which has been demonstrated to be positively associated to breastfeeding initiation17,18. However it was not possible to verify this hypothesis because this specific data was not available in the survey dataset. This singular fact deserves further investigations. Several health-related factors were strongly associated with breastfeeding initiation, some as positive (term births, singletons, breastfed precedent child) and others as negative (obesity, have not breastfed a previous child and no attendance of the public MCH centre) determinants. This data has important policy and clinical implications because some of these factors are manageable for example obesity and attendance of the public MCH centre. In our study, no available social factor was associated to breastfeeding duration (cut-off: six months) while several important social factors such as marital status and income had no effect on breastfeeding behaviours. We were not able to offer a valid explanation to this fact. Finally, this study showed that the main reason for not breastfeeding as reported by the mothers was lack of milk (64.4 percent). This study has several weaknesses. The most important probably include the non specification of the survey’s response rate and the exclusion of the immigrants group. Conclusion Level of breastfeeding initiation rate among Italian women remains rather acceptable (82 percent). Contrary to international literature, our study did not find an association between breastfeeding initiation and some important potential socio demographic determinants (marital status, income etc). Age and employment status were the sole social factors (breastfeeding initiation) identified. Most women continued breastfeeding at least six months after childbirth (63.5 percent). Efforts have to be taken by health-policy makers, healthcare providers and various stakeholders in order to encourage good breastfeeding behaviours. Acknowledgements We are grateful to Professors Francesco Di Stanislao and Emilia Prospero of the Institute of Hygiene and Preventive Medicine of the Università Politecnica delle Marche of Ancona (Italy) for the training provided during the doctorate course and the permission granted to utilize the dataset. References
African Health Sciences Vol 11 No 3 September 2011 The following images related to this document are available:Photo images[hs11101t1.jpg] [hs11101t2.jpg] [hs11101t4.jpg] [hs11101t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}