 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
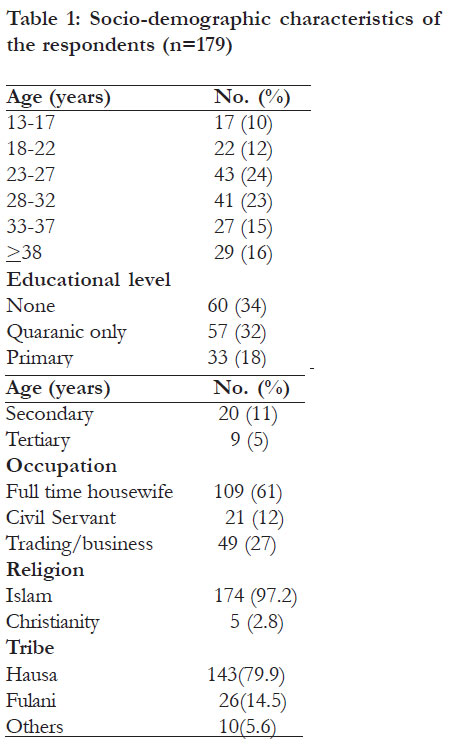
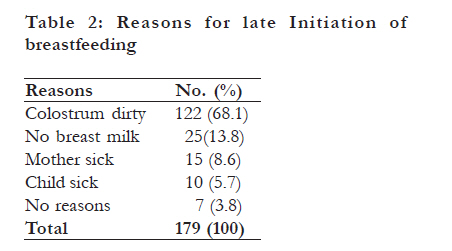
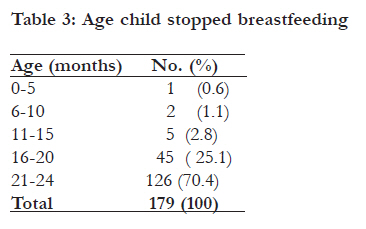
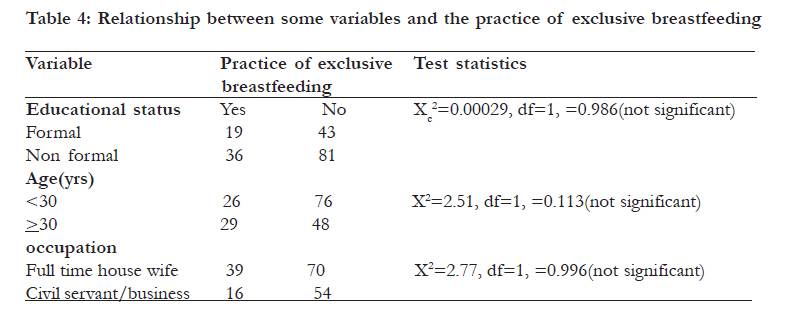
African Health Sciences, Vol. 11, No. 3, Sept, 2011, pp. 518 - 523 Knowledge and practice of exclusive breastfeeding in Kware, Nigeria *Oche MO1, Umar AS1, Ahmed H2 1 Department of Community Health, College of Health Sciences, Usmanu Danfodiyo University, Sokoto, 2 Department of Paediatrics, College of Health Sciences, Usmanu Danfodiyo University, Sokoto Code Number: hs11102 Abstract Background: For almost all infants, breastfeeding remains the simplest, healthiest and least expensive feeding method that fulfils the infants’ needs. Despite strong evidence in support of Exclusive breast feding (EBF) for the first six months of life, its prevalence has remained low worldwide. Key words: Mothers, breastfeeding, knowledge & practice, Kware Introduction For almost all infants, breastfeeding remains the simplest, healthiest and least expensive feeding method that fulfils the infants’ needs.1 The numerous benefits of breast-feeding are of public health relevance for developing countries as well as for industrialized nations. Exclusive breastfeeding, which giving breast milk only and no other liquids, except drops or syrups with vitamins, mineral supplements or medicines, is superior to non-exclusive breastfeeding with a protective effect against both morbidity and mortality 2, 3. Exclusive breast-feeding provides low cost, complete nutrition for the infant, protects him/ her against infections including infant diarrhea, and prolongs lactation amenorrhea, thereby increasing birth spacing4, 5. Despite strong evidences in support of EBF for the first six months of life, its prevalence has remained low worldwide6,7. In Nigeria, breastfeeding is universal with almost all babies being breastfed. However, the practice of EBF is rare with only 17% of children younger than six months being exclusively breastfed. 8 The need to protect, promote and support breastfeeding in our communities has been widely recognised. It is in realisation of this noble objective that the Federal Ministry of Health and Social Services in conjunction with UNICEF and WHO launched the Baby Friendly Hospital Initiative (BFHI) to protect, promote and support breastfeeding in Nigeria. To achieve this objective, a number of Teaching and Specialist hospitals were designated as baby friendly hospitals following the “Innocenti declaration”. The Innocenti Declaration has as its main objectives the promotion of early initiation of breastfeeding (within 30minutes of delivery), EBF for the first six months of life, breastfeeding on demand and continuing breastfeeding with complementary feeds into the second year of life 9, 10. Although several studies have been reported from our study area, these studies however did not assess the knowledge of the mothers with regards to exclusive breastfeeding 11, 12, 13. The objective of this study was to gather information about the knowledge and other factors that influence the practice of EBF in Kware town, a semi urban community in Sokoto State. Method This was a cross sectional descriptive study involving women of child bearing age who were currently breastfeeding at the time of the study or who had stopped breastfeeding not later than two years before (inclusion criterion)while mothers who never breastfed or were temporary visitors to the town were excluded from the study (exclusion criteria). The study took place in Kware town, a semi urban local government area of Sokoto State with 1,350 women of child bearing age.14 The town is served by Comprehensive and Primary health centres in addition to the Federal Neuro-Psychiatric Hospital. The vegetation in Kware town is the guinea Savannah type with an annual rainfall of about 550mm which peaks in August. Dry season sets in first with cold harmattan from October to March and a hot period from April to the end of May when temperature reaches 380C during the day. The main indigenous tribe in the area is Hausa/Fulani with Islam as the main religion. There are other ethnic groups like Ibos, Yoruba, Idomas etc. Farming is the main pre-occupation of the people producing food crops like millet, corn, ground nuts, sorghum and cotton. Animal husbandry is also common among the Fulanis. A sample size of 179 was determined using the formula for cross-sectional studies and a prevalence of EBF of 13%8. A day was set aside for house numbering and using a systematic sampling method, the first of every eight houses was selected from which 179 mother-child pairs were enrolled into the study. Six Community health workers residing in the community were recruited to act as research assistants (RAs). They were trained on the general principles of the research and the study instruments. Data was collected using a comprehensive, pre-tested and structured interviewer-administered questionnaire which sought such information as age, educational status, occupation, initiation of breastfeeding, prelacteal feeding and knowledge and practice of exclusive breastfeeding. Exclusive breastfeeding in this study refers to the practice of giving the infant only breast milk for six months without any fluids except liquid medicines. Knowledge of EBF was assessed through such questions as duration of EBF, feeding the infant with only breast milk for six months; EBF protects the infant against infections etc. The questionnaires were manually sorted out for completeness and accuracy a day after the collection of the data and where there were any omissions; the respondents were traced using the house identification numbers. Data processing and analysis were done using EPI-Info version 3.4.1 computer soft ware programme and Microsoft Office Excel 2003. An author devised scoring and grading system for knowledge was used with each correct answer attracting a mark. A score >50% was graded as adequate knowledge of EBF. Cross tabulation of variables was done where feasible and level of statistical significance was set at 95% confidence interval Ethical considerations Ethical approval was given by the Usmanu Danfodiyo University Teaching Hospital Sokoto ethical committee and a letter of introduction and approval from Kware local government authority to the community leader. Verbal informed consent was obtained from study subjects in their own language explaining the purpose of the study and the right to with draw from it. The respondents were also assured of confidentiality. Results A total of 84 (47%) of the respondents were between the ages of 23-32years while only 29(16%) were above 38 years of age with a mean age of 29.8 ±10.3years. Only 62 (34%), of the study subjects had formal education made up of 33 (18%) Primary, 20 (11%) secondary and 9 (5%) tertiary. All the respondents were married with majority, 109(61%) being fulltime house wives while only 21(12%) of the respondents were civil servants. A total of 143(79.9%) of the women were of the Hausa tribe, with Fulanis constituting 14.5% [Table - 1]. Sixty percent of the mothers were aware of exclusive breastfeeding (EBF) but only 30% of them had adequate knowledge of EBF having scored 50% or more in the assessment of knowledge of EBF. Main Sources of information on EBF were mothers of respondents and health workers. Concerning the breastfeeding practices of the mothers, more than half, 94(53%) initiated breastfeeding immediately (<30minutes) after delivery, while 85(47%) did so long after 30 minutes. Reasons adduced for delayed initiation of breastfeeding among eighty five mothers include colostrum being dirty and thought to be harmful to the child, lack of breast milk and mother or child illness [Table - 2]. For the women who considered colostrum dirty, while awaiting the coming of the clean milk, they gave boiled water, honey, animal milk and washouts from writings of the Quran on slates. A total of fifty-three mothers had stopped breastfeeding at the time of the survey, out of which only one mother stopped breastfeeding before six months due to onset of a new pregnancy, while 45(85%) did so between sixteen to twenty months [Table - 3]. Other reasons for stopping breastfeeding include child old enough to eat family adult food and mother or child’s illness. Out of the 179 mothers, only 55(31%) practiced exclusive breastfeeding. The ages, education and occupation of the respondents were found not to have influenced the practice of EBF [Table - 4]. Discussion In a recent evaluation of the Millennium Development Goals (MDGs), exclusive breastfeeding (EBF) for six months was considered as one of the most effective interventions to achieve MDG-415. In our study, only 54(30%) of the mothers had adequate knowledge of EBF. This is comparable to the study in Gwale, Kano with similar socio-cultural background as the study area, where 31% of the mothers had good knowledge of EBF16. However, the figure obtained in this study is low when compared to the 55% obtained in the study by Freed and his colleagues17 and 98% observed in a similar study in Accra Ghana18. The Baby friendly hospital Initiative (BFHI) was designed to promote early initiation of breastfeeding, preferably immediately after birth. This study observed that 94 (53%) of the mothers initiated breastfeeding immediately after birth. This is higher than 26% and 31% obtained in the studies from Kano and Sokoto respectively16, 19. The study from Western Nepal, India, obtained a higher rate (72.2%) of breastfeeding initiation20. Findings from recent studies have stressed the risk of delayed onset of breastfeeding on neonatal mortality in sub-Saharan Africa and showed that neonatal mortality could be significantly reduced by 16% if the mothers started breastfeeding at day one and 22% when breastfeeding was commenced within the first hour. 21 The major reason for late initiation of breastfeeding in most (47%) of the respondents was colostrum not pure thus supporting the general perception in the study area that in the first three days, the mother’s milk is not pure and therefore could harm the infant. This finding is in consonance with that of Onayande and others in Ile-Ife22 even though the study areas have varying socio-cultural characteristics. While starving the child for the period of not giving colostrum, the child is also denied the benefits of the immunological constituents of colostrum and subsequently delays the proper establishment of lactation later. 23 While awaiting the establishment of the “clean milk”, the mothers gave prelacteals in form of boiled water, honey and animal milk. This is in consonance with findings from similar studies16, 19, 21. The introduction and use of prelacteal feeds have found a common place among African mothers24, 25. In the study community, even though breastfeeding has found universal acceptability with all the mothers’ breastfeeding their infants, the exclusive breastfeeding (EBF) rate was found to be only 31%. The EBF rate obtained in this study was however high compared to 17% reported for Nigeria in the Nigerian Demographic and Health survey8 and equally higher than figures obtained in other studies16, 26, 27, 28. In contrast to the EBF rate obtained in this study, Oche19, in a separate study in the same zone as the study area, obtained an EBF rate of 79%.The high rate obtained in his study may not be unconnected with the fact that all his subjects were full time house wives and therefore had enough time to carry on breastfeeding for longer periods. Maternal education is related to knowledge of good child care practice and to household wealth. Female education has severally been described as one of the strongest determinants of the practice of EBF29. In our study, education of the respondents had no influence on the practice of EBF as there was no statistically significant difference between those with formal education and informal education with regards to the practice of EBF (p=0.986). Although, 39 housewives compared to 19 civil servants practiced EBF, this was found not to be statistically significant (p=0.096). This is in contrast to another study in the same study area where the authors opined that the high rate of EBF by the mothers could be attributed to their being full time housewives and therefore they had enough time to practice EBF19. Only 1(2%) subject stopped breastfeeding before six months which is in consonance with the study from Kano, where 2.4% of the respondents stopped breastfeeding before the age of six months. 16 The only mother that stopped breastfeeding before six months did so because of the onset of a new pregnancy. In the study area, the widely held cultural belief is that the new pregnancy produces milk that is contaminated and thus harmful to the child hence the need to put the child off the breast. This practice has far reaching implications for the growing children as they are exposed to malnutrition and denied all the benefits of breastfeeding. The commonest reason for stoppage of breastfeeding in this study was that the child was old enough and could eat solid foods. This is in consonance with the findings from another study in Sokoto State. 19 Limitations The study did not explore other cultural determinants of breastfeeding which might have some influence on EBF. Conclusion Even though breastfeeding has found universal acceptability in the study area as evidenced by the fact that all the children were breastfed, the knowledge and practice of EBF is abysmally low. To achieve the goals of the MDG-4, there is the need to institute intervention measures aimed at increasing EBF rates in the study community. Appropriate education directed at early initiation of breastfeeding, improved knowledge of EBF and use of colostrum is required to enhance EBF and duration of breastfeeding. Acknowledgements We wish to thank Hajia Hauwa, Maryam and Saratu for the data collection. Our appreciation goes to the Department of Primary Health Care of the Kware local government area for giving us the permission to carry out the study and also the mothers of kware town for agreeing to participate in this study. References
African Health Sciences Vol 11 No 3 September 2011 The following images related to this document are available:Photo images[hs11102t2.jpg] [hs11102t3.jpg] [hs11102t1.jpg] [hs11102t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}