 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
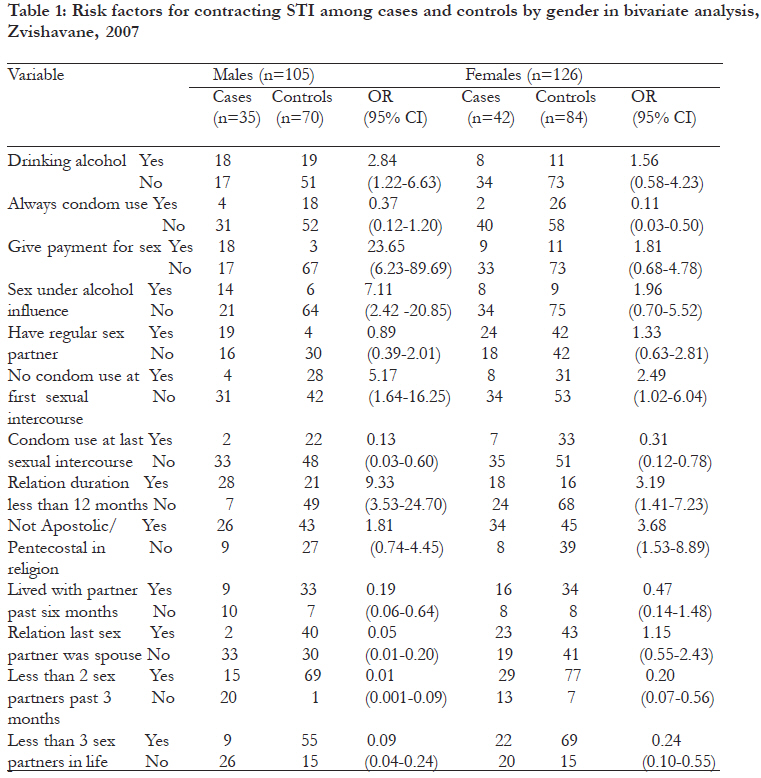
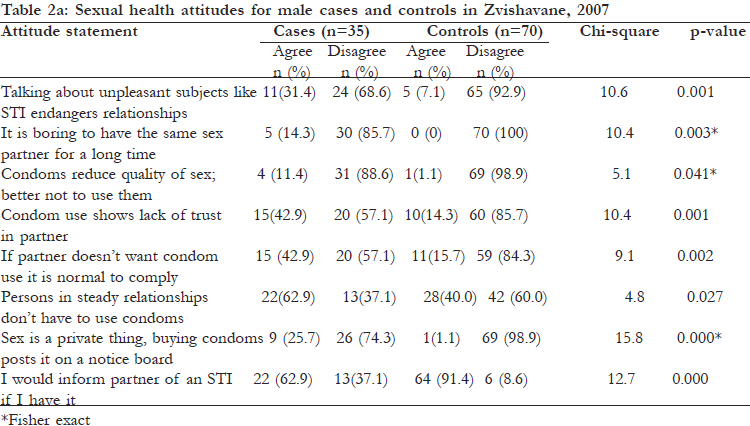
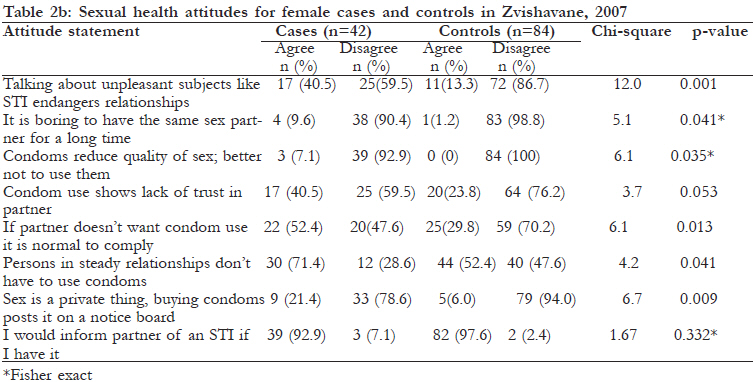
African Health Sciences, Vol. 11, No. 4, Dec, 2011, pp. 535-542 Factors associated with contracting sexually transmitted infections among patients in Zvishavane urban, Zimbabwe; 2007 *Chadambuka A1, Chimusoro A2, Maradzika JC1, Tshimanga M 1, Gombe NT1, Shambira G1 1. Department of Community Medicine- University of Zimbabwe Code Number: hs11109 Abstract Background: Sexually transmitted infections (STIs) remain a major public health problem in Zimbabwe. In Zvishavane, STI increased from 66 per 1,000 in 2002 to 97 per 1,000 in 2005, a 31% increase in cases. Key Words: Zvishavane, sexually transmitted infection, transactional sex Introduction Sexually transmitted infections (STI) remain a public health problem worldwide. Transmission is through person to person during intercourse. Contracting STI has implications for the patient and partner which include infertility, and human immunodeficiency virus (HIV) infection/acquired immunodeficiency syndrome (AIDS) 1. A strong correlation exists between STI and HIV transmission. STIs like gonorrhea, genital ulcers, urethral and vaginal discharge increase the risk of sexual transmission of HIV by 5-12 times 2-4. World Health Organization (WHO) estimates 340 million cases of sexually transmitted infections occur annually worldwide. In developing countries, they rank among the top five diseases for which adults seek care 5. Risk factors for STI that have been documented include unprotected vaginal, anal and oral sex, close skin to skin contact with infected areas, sex with strangers or commercial sex workers, multiple sex partners, injection drug use or sex with injection drug users, and sharing needles for body piercing and tattoos.6 Knowledge of where to obtain condoms and not discussing family planning with a partner have been cited as risk factors among women7, and low knowledge of STI complications has been associated with the practice of multiple sexual partners and not using condoms with casual partners 8. Very few studies have looked into attitudes towards STI preventive health behaviours9. In Zimbabwe, STI account for 6-10% of outpatient attendances. Sites of high STI prevalence were associated with majortransport routes. Gender segregated labour migration was amajor contributor to STI transmission risk in Zimbabwe10. In Zvishavane, STI were among the top five causes of outpatient consultations among adults11-12. The majority (51.2%) of cases came from three urban health facilities, and the remainder from 16 rural facilities12. Statistics showed a continual increase in STI cases, from 66 per 1,000 in 2002 to 97 per 1,000 in 200511, a 31% increase in STI cases. The magnitude of the problem was likely to be higher as STI patients often sought care from private providers, from who there is no data. We investigated risk factors for STI in Zvishavane. Methods A 1:2 case control study was conducted in Zvishavane urban. The urban setting has a total of three health facilities, a government hospital, a mine hospital, and a council clinic. Cases were frequency matched for age and sex to controls. A case was any person above 15 years diagnosed with STI at three health facilities in Zvishavane urban from 18 June to 8 July 2007. Diagnosis of STI was made using the syndromic approach. Controls were sexually active patients (same sex with case) within a five year age group of the case, who visited the same facilities for other ailments. Cases and controls were recruited by trained research assistants as they reported to the health facilities. All patients diagnosed with STI (cases) were invited to participate. Controls were the first two patients who met matching criteria and who reported to the same health facility after an eligible case. The study population was sexually active people (those who had sex at least once in the previous three months) in Zvishavane urban. We conducted the study at three health facilities: two hospitals and one clinic. We assumed 44% of the cases reporting regular alcohol use in sexual encounters13 and an odds ratio of 2.6 at 95% confidence and 80% power. We calculated a sample size of 60 cases and 120 controls, adjusted for 20% non response to obtain a sample size of 75 cases and 150 controls. A total of 82 cases were eligible for participation. The number interviewed were 77 cases and 154 controls. Refusal rate was 6.5% among cases and 5.2% among controls. We used interviewer administered questionnaires to collect demographic data, data on knowledge of sexually transmitted infection and risk factors. We assessed attitudes towards preventive health behaviours. We generated 12 items to assess attitudes and pre-tested them on 25 patients to generate Cronbach’s alpha using STATA (a measure of the reliability of the items in accurately measuring attitude). A high alpha is an indication that the items are measuring a unitary construct i.e. attitude. Statements coded from strongly agree to strongly disagree were recoded into agree and disagree for bivariate analysis. We generated frequencies, median, odds ratios and chi square. We performed logistic regression for independent risk factors. Data was examined separately among males and females. We reported on eight of the twelve attitude statements which had statistically significant differences. Ethical review committees of the three institutions approved the study protocol. Permission to conduct the study was obtained from the Provincial Medical director and Medical superintendents for the hospitals. Participants gave verbal consent to be interviewed in the study. No invasive procedure was done. Infected persons were treated free of charge and counseled on site. No names were captured in order to preserve anonymity. Results The median age for male cases and controls was 27 (Q1=24; Q3=34) and 29 (Q1=24: Q3=33) respectively. The median age for female cases and controls was 26 (Q1=24; Q3=28) and 29 (Q1=23: Q3=29) respectively. The median age at sex debut for male cases and controls was 20 (Q1=19; Q3=21) and 20 (Q1=19: Q3=22) respectively. The median age at sex debut for female cases and controls was 18 (Q1=17; Q3=20) and 19 (Q1=17: Q3=21) respectively. Except for religion (male cases and controls: chi square=1.71, p=0.19; female cases and controls: chi square=8.98, p=0.002), there were no significant differences ( chi square test) in marital status, educational level, and unemployment between cases and controls, for both males and females. Knowledge of STI Similar proportions (35 (100%) and 41 (98%)) of male and female cases had heard about STI, compared to 69 (99%) and 83 (99%) of male and female controls respectively. A correct definition of STI was given by 96.1% of cases and 98.1% of controls. Similar proportions of cases (98.7%) and controls (100%) knew STI were contracted through unprotected sex for both males and females. There was no difference in knowledge of prevention methods between males and females. Most controls (80.5%) reported receiving information from health workers as compared to 57.1% cases (p=0.000). Types of STI The most common STI diagnosed in men were urethral discharge (65.7%), genital ulcer (17.4%), and inguinal swelling (11.6%). Among women, the most common STI diagnosed were vaginal discharge (40.8%), pelvic inflammatory disease (19.4%), lower 9.33 (95% CI 3.53-24.70), no condom use at first abdominal pain (16.8%) and genital ulcers (14.4%). Risk Factors for STI With reference to [Table - 1], risk factors for males were alcohol consumption OR 2.84 (95% CI 1.22-6.63), sex under the influence of alcohol OR=7.11 (95% CI 2.42-20.85), relationships less than 1year OR=9.33 (95% CI 3.53-24.70), no condom use at first intercourse OR=5.17 (95% CI 1.64-16.25) and paying for sex OR=23.65 (95% CI 6.23-89.69). For females the risk factors were non-use of condom at first intercourse, OR=2.49 (95% CI 1.02-6.04) and relationships less than one year OR=3.19 (95% CI 1.41-7.23). Protective factors for males were having only one and having wife as last sex partner, OR=0.05 (95% sex partners in in last three months OR=0.01 (95% CI 0.01-0.20). Protective factors for women were CI 0.001-0.09), <3 sex partners in life OR= 0.09 having only one sex partner in last three months (95% CI 0.04-0.24), condom use at last intercourse OR=0.20 (95% CI 0.07-0.56), <3 sex partners in OR=0.13 (95% CI 0.03-0.60), living with sex partner life OR=0.24 (95% CI 0.10-0.55), condom use at previous six months OR=0.19 (95% CI 0.06-0.64), last intercourse OR=0.31 (95% CI 0.12-0.78), always using condoms OR=0.11 (95% CI 0.03-0.50) and being pentecostal/apostolic in religion, OR=0.27 (95% CI 0.11-0.66). Multivariate analysis Stepwise logistic regression was conducted separately for men and women due to interaction of many factors by gender. Independent factors associated with STI were belonging to pentecostal/apostolic religion, (AOR = 0.35, 95% CI 0.13-0.92), having more than one sex partner in the past three months (AOR = 4.45, 95% CI 1.50-13.17), having a relationship of more than one year with last partner (AOR = 0.3, 95% CI 0.1-0.94) and using a condom during last sex (AOR = 0.26, 95% CI 0.09-0.73) for women. For men, independent factors were using a condom during last sex (AOR = 0.14, 95% CI 0.02-0.89), having more than one sex partner in the past three months (AOR = 50.5, 95% CI 3.46-736) and having last sexual relation with spouse (AOR = 0.02, 95% CI 0.0020.12). Attitudes We assessed attitudes using 12 statements (Cronbach alpha =0.79). Male cases and controls had significant differences in attitudes towards all sexual health attitude statements [Table - 2a]. A similar picture was evident for female cases and controls except in one attitude statement [Table - 2b]. Discussion Knowledge of STI Knowledge of STI Knowledge of STI was high in the study population although it did not translate into safe behaviour. prevention of STI including using condoms as means of protection was well known but in practice, reported condom use was low for both cases and controls, reflecting a discrepancy in knowledge and practice. Studies have shown no relationship between knowledge and behaviour. Behaviour is related to perceptions that people have which they use to make judgments14, 30. Risk factors This study found more men than women reported having last sex with non-regular partners. Men are more likely to have multiple partners or casual partners than women15-17. Having one’s spouse as the last sex partner was protective for males but not for females. Male partners are more likely to have had unprotected sex outside the marriage thus predisposing their partners to STI. Colvin et al observed the same in a rural community in the Lesotho highlands18. Ndubani et al revealed that perceptions of manhood encouraged multiple sexual relationships19. Silberschmidt. found Gusii men boast of having many wives or girlfriends. Having multiple partners may be perceived as virility and demonstrates maleness in this community20. Women in this study conceded to sex the previous three months but most could not decline sex without a condom. Women’s lack of power in their sexual relationships put them at risk for reproductive infections. Women are put at potential risk for STI and HIV by their husbands’ risky sex behavior. This agrees with the findings of Shelah et al who studied behaviour of husbands and the wives’ risk of STI and HIV21. Asamoah-Odei showed that even when women knew their spouse had several partners, most lacked the power to negotiate for safer sex22-25. Relationships of less than one year’s duration were associated with STI. This reflects that sex was of a high risk if duration of the relationship was less than one year. Partners were likely to be multiple and infected with STI in such scenario. Men who had their spouse as a last sex partner of experienced a protective effect. In general men tend to engage in sex with commercial sex workers or casual acquaintances more than women. It is highly likely that those who had last sex with their spouse alsolived together with their spouse and were both faithful decreasing the risk of contracting STI. This study shows that condom use during the last intercourse was higher among the controls and was protective. The fact that controls enjoyed less risk shows condoms are effective. Work on changing fears, attitudes, and misconceptions that lead to people not using condoms is critical. Such attitudes include fear of condom failure, associating condom use with promiscuity, the perception that there is no need to use condoms in a steady relationship and erection loss26. Being pentecostal or apostolic was found significantly protective against STI among women contrary to the findings of Shendre et al (2002). These religions condemn adultery and fornication and members are excommunicated for such behaviour. The belief in the norms of these institutions and desire to conform affords members protection as they are perhaps less likely to engage in activities that their religion condemns27. Sanchez et al (1996) found religion as an insignificant risk factor 28. The protective effect could also be due to cases being less likely to report belonging to pentecostal religion once diagnosed with STI or less likely to seek care for that problem if Apostolic as some Apostolic religions prohibit treatment seeking in their teaching. They were more likely to use condoms and have fewer sex partners. Living with one’s partner in the past six months and having one’s last sex partner as spouse was protective, because individuals seek gratification from their spouses or live-in partner. For those in a steady and faithful relationship, the likelihood of acquiring a STI infection is minimal. Attitudes Both male and female cases and controls had significant differences in attitudes. Case patients had more negative attitudes towards condom use. Condoms may be associated with promiscuity and infidelity. They may be seen as objects used only during ‘hit and run’ sexual relationships, but never in stable sexual partnerships. This is evidenced by significantly higher STI risk among those who agreed with the statements, “condom use shows lack of trust in partner” and “people in a steady relationship do not have to use condoms”. The study found that cases expressed willingness to inform partners if they were infected with a STI. Informing sexual partners about STI has protective effects and is advocated for to facilitate the treatment of both the index case and contacts to avoid re-infection or prevent infecting the partner. This is in agreement with what Ndubani et al found among Zambian men. A few disagreed as they feared creating disharmony in relationships19-20. This study found 9.1 % of individuals with STI had the attitude that a condom reduces the quality of sex. Having that attitude may make the likelihood of condom use remote as the primary objective for sex is gratification. Musa (1997) found that 68% of respondents reported that condoms spoiled sexual pleasure and did not want to use them.29 Those who felt buying condoms was like publicizing sex may not buy them despite knowledge of the risks and they may proceed to engage in unprotected sex. Trigg et al (1997) found embarrassment in procuring condoms strongly associated with risky sexual behaviour30. To encourage people to use condoms, awareness of HIV/STI risks should be raised, make good-quality condoms readily available, teach people how to use condoms correctly, work to eradicate the social stigma associated with condoms, and advocate for HIV prevention and condom use in the community. The condom awareness or outreach programmes must be defined at the level of the community and in association with the community. The use of problem-solving techniques for selecting the most relevant attitudes, based on their importance and changeability, should be employed31. For example, counseling could help clients assess their risk of infection and create a risk reduction plan, address misconceptions, attitudes and rumours, teach condom use and negotiation skills, help clients deal with problems using condoms, and refer condom clients for other services. The national and local policies about condoms affect acceptability, as much as attitudes and pronouncements about condom use by parents, church leaders, peers, entertainment figures, and political leaders32. Promotional programmes should engage influential people and make them publicly speak positively about condom use. People are more likely to model their behaviour around that shown by those who have influence over them. The factors that affect acceptability of condoms can be thought of as a series of concentric circles that interact with each other — from the individual at the centre to the couple, the health-care system, the community, and the entire world. An individual’s knowledge, attitudes, habits, perceptions, awareness of the need, and other internalized factors, are critical to condom use. But what forms those belief systems and determines individual behavior? The dynamics between sexual partners play a crucial role and depend on many factors, such as whether sex is with a regular partner or not, whether the couple talks about sex and protection against disease and unwanted pregnancy, and whether sex is voluntary for both parties. Behavior change thus involves many issues, and before that can occur, people have to change attitudes, such as acknowledging their risk of infection. People need knowledge on what causes STI and HIV transmission, what types of sexual behaviours can put a person at increased risk of infection, and how to change those attitudes and behaviors. They need skills to communicate with a partner about the importance of condom use. To take the next step and begin using condoms, people must find condoms readily available and affordable32. Study limitations The cases were not randomly selected. Cases and controls were matched by age using a 5-year window, but an age difference of five years could be large for adolescent participants. Differences of one year confer large developmental differences that could impact on study variables. Resources were inadequate to use the largest sample size possible. Self reported information was relied on. Recall bias in reporting numbers of sex partners, over and under-reporting of partners between sexes cannot be excluded. Bias arising from knowing interviewers were health workers and conducting the study from the health facility cannot be ruled out. Conclusion Limiting the number of partners, consistent condom use, and fidelity are important for both men and women. Attitudes towards condom use need to be improved. Recommendations The STI coordinator should focus on and strengthen behaviour change communication with respect to promotion of condom use and promotion of lasting relationships. The health promotion officer should develop materials which reduce stigma associated with condoms and address sexual health attitudes. Acknowledgement I would like to acknowledge support of staff at the three institutions that participated in the study, and all the study participants for making this study possible References
Copyright © 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11109t2a.jpg] [hs11109t1.jpg] [hs11109t2b.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}