 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
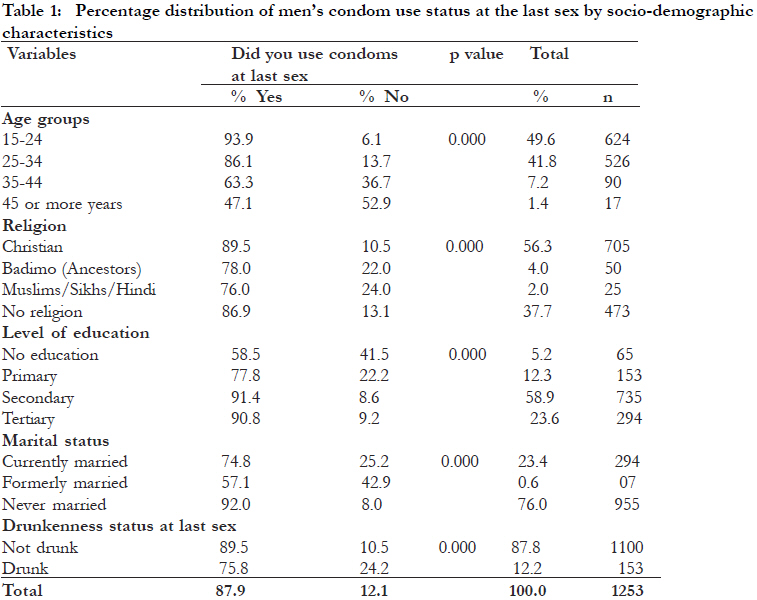
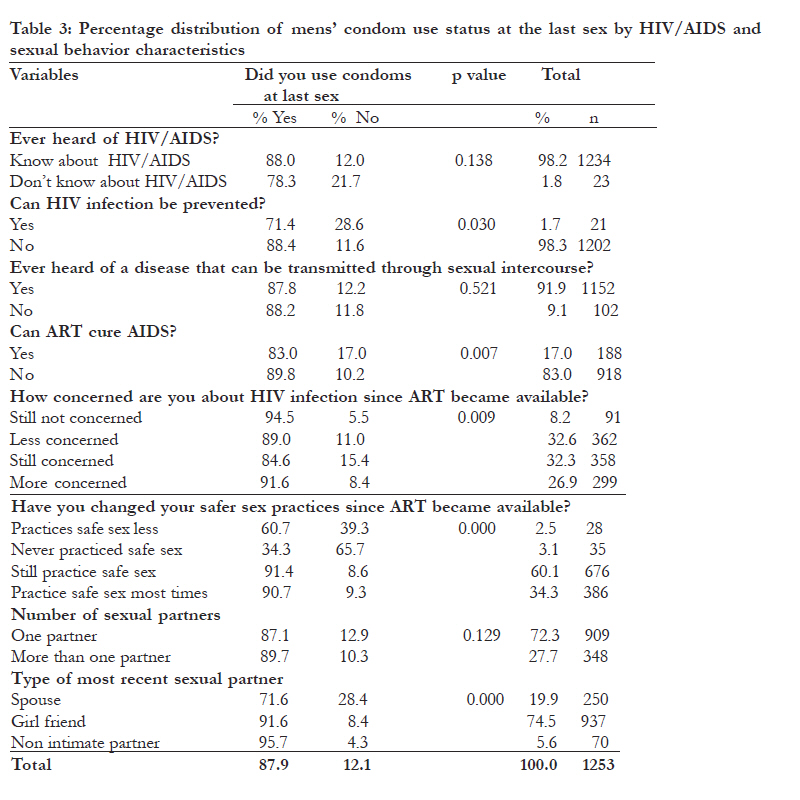
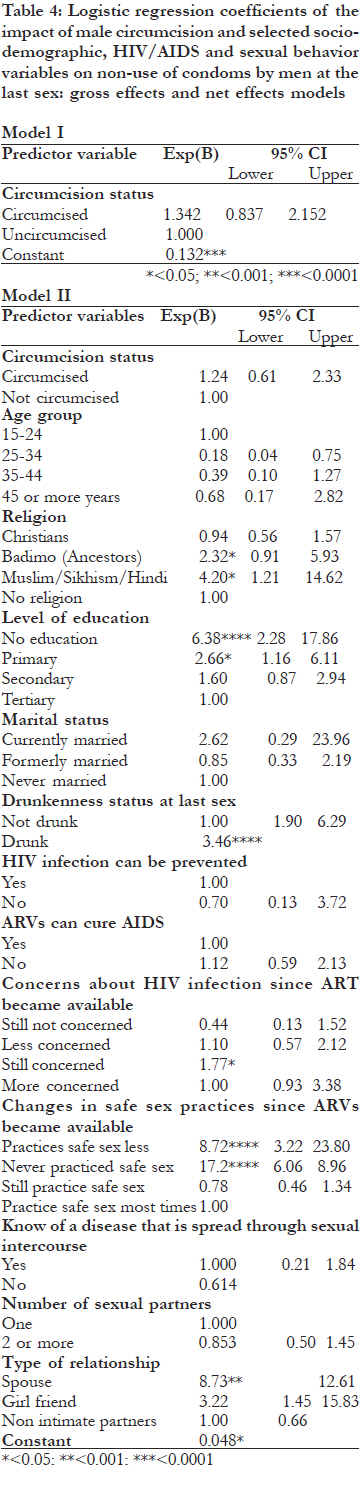
African Health Sciences, Vol. 11, No. 4, Dec, 2011, pp. 550-559 Impact of male circumcision on HIV risk compensation through the impediment of condom use in Botswana *Ayiga N 1, Letamo G 2 1 Population Training and Research Unit, North West University Mafikeng Campus, Private Bag x2046,Mmabatho 2735, South Africa Code Number: hs11111 Abstract Background: Male circumcision has been recommended as a method of reducing the risk of transmitting HIV. However, widespread uptake of male circumcision may lead to HIV risk compensation by impeding condom use. Key words: male circumcision, condom use, Botswana Introduction Circumcision is probably one of the oldest of all surgical procedures. Male circumcision was believed to have started as a religious rite and continues to be so among Jews and Muslims. Among Jews, circumcision also known as “Bris Milah” is performed on the eighth day after birth and among Moslems “Tahara” meaning purification is usually performed in childhood. Christianity remained ambivalent to male circumcision and it was neither prevented nor encouraged 1. In the developed world, male circumcision is performed for medical reasons 2 and in sub-Saharan Africa, some societies circumcise as a rite of passage from childhood to adulthood 3. In Botswana male circumcision was historically practiced as an initiation to mark the transition from boyhood to manhood also known as “Bogwera” and to protect against balanitis before it was generally abandoned during colonialism 4. Knowledge that male circumcision could prevent HIV transmission to males is relatively new having been first proposed by Alcena 5, who postulated that removing the foreskin of males can prevent HIV transmission from females to males. Anthropological and epidemiologic studies in sub-Saharan Africa have also suggested that HIV infection is lower among circumcised men 6, 3, 7, 8. Despite these observations, the use of male circumcision as a method of preventing HIV transmission was not widely accepted until the randomized control studies in South Africa 9, Kenya 10 and Uganda 11. These studies found that uncircumcised men contracted HIV more easily than circumcised men. However, the extent to which male circumcision could reduce HIV transmission to males remains a matter of debate and is controversial. Some opponents argue that the conclusions and recommendations from the South African, Kenyan and Ugandan studies were premature 12. Others 13,14 suggested that male circumcision alone may not prevent HIV transmission, especially in the context of multiple sexual partnerships, which is a tolerated high risk behaviour in some cultures and religions. HIV infections have also been found to occur in individuals who are circumcised 9,15. As a result of the above and other findings many anti-HIV/AIDS activists have argued that wide spread male circumcision in a high HIV prevalence population could lead to risk compensation and transmission of HIV 16. Male circumcision is also unlikely to reduce HIV incidence rates where knowledge of HIV/AIDS status is low and resistance to HIV counseling and testing is still strong. This could increase the risk of HIV transmission to females who are HIV negative or whose HIV status is unknown and are having sex with circumcised men. Up scaling male circumcision should therefore be accompanied by HIV prevention education, counseling, and behaviour change interventions, including sustained promotion of condom use 17,18. The Ministry of Health in Botswana has already started rolling out male circumcision and its target is to circumcise 80% of all eligible males by 2012 19. This is possible because 81% of Batswana men are willing to circumcise if it were free, safe, and performed in a health facility 20. The concern is that male circumcision could change the current perceptions and attitudes of males and females towards protected sexual intercourse by impeding use of condoms. Evidence on whether circumcision could increase HIV risk compensation by impeding use of condoms is not yet well known. This study therefore investigated whether or not male circumcision impedes condom use, by comparing condom use at the last sex among circumcised and uncircumcised men. Methods Data used in this study were obtained from the Botswana AIDS Impact Survey (BAIS) III which was conducted in 2008. The survey was conducted by the Central Statistical Office (CSO) in collaboration with the National AIDS Control Agency (NACA) of the Republic of Botswana. The BAIS III was a cross-sectional survey and it used a stratified two-stage sample design to draw its sample21. The main objective of the survey was to provide up-to-date information on the HIV/AIDS pandemic in Botswana with respect to its prevalence, behavioural patterns, care and support, and stigma. Respondents to the individual questionnaire were males and females aged 10-64 years. However, in these analyses, data on male respondents aged 1564 years who fully completed the individual questionnaire, and were sexually active were used. Ethical clearance was obtained from the BAIS III Reference Group at NACA. Informed consent was obtained from individuals who voluntarily accepted to participate in the study. They were assured of their right to withdraw from the study if they so wish and that such withdrawal will not affect their rights to health and other services. Data were collected from the consenting individuals anonymously. The dependent variable is condom use at the last sexual intercourse. The main explanatory variable is circumcision status of men. Data on age at circumcision, whether circumcision was traditionally or medically performed and the willingness to circumcise were used as control variables. Socio-demographic data on current age, religion, level of education, marital status, and drunkenness status at the last sexual intercourse were also used as control variables. In addition, data on HIV/AIDS and sexual behavior used in this analyses included knowledge of HIV/AIDS, whether or not HIV infection can be prevented, whether or not ART can cure AIDS, concerns about HIV infection since ART became available, personal safe sex practices since ART became available, knowledge of diseases that could be transmitted through sexual intercourse, number of sexual partners and type of last sexual partner. Statistical Analysis The Pearson’s chi-square statistics ( x2) was used to test for the association between condom use as the dependent variable and circumcision status, sociodemographic, HIV/AIDS and sexual behaviour characteristics as explanatory variables using the 95% confidence interval (CI). The effect of male circumcision on condom use was further examined by using the binary logistic regression without controlling for the effect of socio-demographic, HIV/AIDS and sexual behaviour characteristics in model I, and after controlling for the effects of sociodemographic, HIV/AIDS and sexual behaviour characteristics in model II. The binary logistic regression method was chosen because the dependent variable is binary and the explanatory variables are categorical22. The model used to measure the probability of not using condoms is given by log [P/ (1- P)], where P is the probability of not using condoms at the last sexual intercourse. Results Description of the sample [Table - 1] presents the distribution of respondents by socio-demographic characteristics. The table shows that nearly 50% of the men were under 25 years; 41.8% were 25-34 years; and only 8.6% were 35 years or older. Fifty six percent of respondents were Christians, 37.7% had no religion, and 4% and 2% were “Badimo” which means believers in ancestral spirits, a form of African traditional religion (ATR), and Muslims/Sikhs/Hindi respectively. Nearly 6 out of 10 respondents attained secondary education, 23.6% attained tertiary education, 12.3% had primary education, and only 5.2% had no education. About 76% were never married, 23.4% were currently married, and nearly one percent was formerly married. Only 12.2% said they or their partner was drunk at the last sexual intercourse. In [Table - 2] the circumcision characteristics of the sexually active men are presented. The table shows that only 12.9% of the men were circumcised. Of those circumcised, nearly 47% were circumcised at birth, 47.8% were circumcised later in life, and 5.7% did not know the age at circumcision. Nearly 73% were circumcised in health facilities, 19% were circumcised traditionally, and about 8% did not know the circumstances of circumcision. Additionally, 77% of those who were not yet circumcised were willing to be circumcised if the procedure could reduce the risk of STIs. The HIV/AIDS and sexual behaviour characteristics of the men are presented in [Table - 3] indicating that knowledge of HIV/AIDS (98.2%) and knowledge that HIV infection can be prevented (98.3%) were nearly universal. Ninety two per cent of the men knew the diseases that can be transmitted through sexual intercourse and 83% knew that antiretroviral treatment (ART) cannot cure AIDS. Nearly 27% of the men said they were more concerned, 32.3% said they remained concerned, and 32.6% and 8.2% said they were less concerned and not concerned at all respectively about HIV since ART became available. Just over 60% of the men still practiced safe sex, 34.1% practiced safe sex more than ever, and only 3.1% and 2.5% never practiced safe sex became available. and practiced safe sex less respectively, since ART becomes available. Regarding sexual behaviour, nearly 3 in 10 men had recent sexual partner was a girlfriend and a spouse multiple concurrent sexual partners. Additionally, respectively. Only 5.6% said their recent sexual partner 74.5% and nearly 20% of the men said their most was a non intimate partner. Differentials in non-use of condoms at the last sexual intercourse Differentials in non-use of condoms at the last sex by socio-demographic characteristics are presented in [Table - 1]. The table shows that non-use of condoms was more likely among older men. Nearly 53% and 37% of men aged 45 or more years and 35-44 years respectively did not use condoms at the last sexual intercourse. Muslims/Sikhs/Hindi (24%) and Badimo (22%) were also more likely not to have used condoms compared to Christians (10.5%) and those with no religion (13.7%). Regarding the level of education, 41.5% and 22.2% of the men with no education and with primary education respectively did not use condoms at the last sexual intercourse compared to 8.6% and 9.2% of those with secondary and tertiary education respectively. Additionally, the formerly married (42.9%), currently married (25.2%), and over 24% of men who reported that they or their partner was drunk at the last sexual occasion also did not use condoms. Age, religion, level of education, marital status and drunkenness were significantly associated with non-use of condoms at the last sexual intercourse at 99% CI. In [Table - 2], differentials in condom use at the last sexual intercourse is presented by circumcision status, age at circumcision, place of circumcision and willingness to circumcise. The table shows that nonuse of condoms was higher among circumcised men (15%), those circumcised later in life (19.7%), and those circumcised traditionally (20%). Non-use of condoms was also higher among men who said they would circumcise if it could reduce risk of STIs (12.7%). However, circumcision status, age at circumcision, place of circumcision and willingness to circumcise were not significantly associated with non-use of condoms at the last sexual intercourse. The association between HIV/AIDS and sexual behaviour characteristics and non-use of condoms is presented in [Table - 3] indicating that nonuse of condoms at the last sexual intercourse was higher (28.6%) among men who said HIV transmission can be prevented and those who believed ART can cure AIDS (17%). Just over 15% of men who remained concerned and 11% of men who were less concerned about HIV infection after ART became available did not use condoms at the last sexual intercourse. Non-use of condoms was even much lower among those who were not concerned (5.5%) and more concerned (8.4%) about HIV infection since ART became available. The majority (65.7%) of men who never practiced safe sex, followed by those who practice safe sex less (39.3%) did not use condoms at the last sexual intercourse. Only 8.6% and 9.3% of men who said they still practice safe sex and practice safe sex most times used condoms at the last sexual intercourse. Regarding the type of most recent sexual partner, as expected, the majority (28.4%) of men who had the last sex with spouses did not use condoms. Nonuse of condoms was significantly associated with whether or not HIV infection can be prevented, whether or not ART can cure AIDS, concerns about HIV infection after ART became available, changes in safe sex practices after ART became available, and type of partner at the last sexual intercourse. Predictors of non-use of condoms The predictors of non-use of condoms at the last sexual intercourse are presented in [Table - 4]. Model I presents the gross effect of circumcision on nonuse of condoms. The result shows that circumcised males were 1.3 times more likely not to have used condoms at the last sexual intercourse than uncircumcised men. In Model II the effect of circumcision on non-use of condoms at the last sexual intercourse after controlling for the effects of selected socio-demographic, HIV/AIDS and sexual behaviour characteristics shows that circumcised men were 1.2 times more likely not to have used condoms than uncircumcised men. In both models, circumcision status was not significantly associated with non-use of condoms at the last sexual intercourse. However, some of the control variables were found to be significantly associated with nonuse of condoms at the last sexual intercourse. Nonuse of condoms on this sexual occasion was more likely among Muslim/Sikhs/Hindi (OR 4.20, CL 1.21-14.62); and Badimo followers (OR 2.32, CI 0.91-5.93). Having no education (OR 6.38, CI 2.2817.86) and having primary education (OR 2.66, CI 1.16-6.11) were significantly associated with non-use of condoms at the last sex. Also significantly associated with non-use of condoms at the last sexual intercourse were being drunk (OR 3.46, CI 1.906.29); practicing safer sex less since ART became available (OR 8.72, CI 3.22-13.80); never practicing safer sex since ART became available (OR 17.2, CI6.06-8.96); and having the last sex with spouses (OR 8.73, CI 1.45-12.61). Discussion At 17.6% 21, Botswana has one of the highest adult HIV/AIDS prevalence rates in the world. It has been in the fore front of reducing further spread of the infection and mitigating the health and socioeconomic impacts of the disease through several programs including ABC, PMTCT, and ART 23. The country has recently adopted and started implementing a country wide circumcision programme as another strategy of preventing HIV transmission to men. The objective is to circumcise 80% of all eligible men by 2012. However circumcision has increased fears of upping risky sexual behaviour through a decrease in perceived risk also known as HIV risk compensation by impeding condom use by circumcised men. This study therefore investigated the impact of male circumcision on non-use of condoms by comparing circumcised men with uncircumcised men. The results of this study showed that overall, circumcised men were more likely to have not used condoms at the last sex than uncircumcised men. However, non-use of condoms and circumcision were not statistically associated implying that male circumcision did not impede condom use in Botswana. The study found that non-use of condoms continues to be impeded by religious beliefs, lack of or low education, drunkenness, misconceptions about ART and type of sexual partner. The finding regarding the impact of circumcision on non-use of condoms is consistent with a previous study24, which found that male circumcision did not increase risky sexual behaviour. This could be attributed to continued HIV education in Botswana where a large number of circumcisions are performed later in life. Furthermore, the demand for circumcision has soared since its introduction as an add-on method of preventing STIs including HIV transmission and is performed in health facilities across the country. The higher rate of non-use of condoms at the last sexual intercourse observed in this study by people with no or low education has also been observed in previous studies25–28. These studies found that condom use increased with the level of education. Greater use of condoms by people with higher education could result from their more liberal outlook to sexual behaviour; better knowledge about condoms and where they could be obtained; and better understanding of the importance of condoms in preventing STIs including HIV. Although not significant at the multivariate level for the currently married, but significant for those whose last sexual intercourse was with a spouse, we found that non-use of condoms was more likely in marriage, which we did not consider surprising and is consistent with previous studies29-31. In Botswana as in most of sub-Saharan Africa, the condom has mostly been promoted as a disease prevention method for people who engage in casual sex, commercial sex, and unstable and short term relationships. As a result using condoms with spouses has always been problematic and viewed with mistrust. Besides, married people and those in stable unions perceive themselves not to be at risk of HIV infection. The promotion of condoms for use within marriage as a safe sex practice is most unlikely to succeed because of its direct imputation of mistrust. The higher rate of non-use of condoms in the state of drunkenness in this study also agrees with the findings of previous studies 31,32-34. These studies found that drunkenness is associated with risky sexual behaviour characterized by frequent sexual activity and multiple sexual partnerships. This is because drunkenness increases sexual desires, reduces reasoning skills and contributes to poor judgement because of impaired ability to make correct decisions. This leads to sexual activity even in the most bizarre manner and rape which is inconsistent with use of condoms. These effects of alcohol were found to apply similarly to men who use alcohol regardless of their circumcision status 34. The higher sexual risk taking after using alcohol could also be a result of what may be described as alcohol expectancy for condom use behaviour 35. Religious beliefs can impact on HIV dynamics in a number of ways including non-use of condoms. This study found that religious beliefs are significantly associated with non-use of condoms. Muslims/Sikhs/Hindi and Badimo men were significantly less likely to have used condoms at the last sexual intercourse. Among Muslims/Sikhs/ Hindi, non-use of condoms could be attributed to the emphasis of faithfulness within marriage and the prohibition of premarital and extramarital sex which is the main basis for condom use 36. Islam also prohibits the use of alcohol, which has been found to contribute to non-use of condoms37. On the other hand, non-use of condoms by the believers in ancestral spirits “Badimo”, could be encouraged by the perception that condom use contravenes their sexual values and the sacredness of sexual intercourse, which has been suggested in another study38. In all religions sexual behavior is highly regulated and prescribed, including ATR. The perception that HIV/AIDS is a consequence of deviating from valued sexual norms is not uncommon 39. This perception may have motivated Badimo men who adhere to their sexual norms not to use condoms. Before ART became available, the ABC strategy was the main HIV/AIDS prevention method. The ABC strategy has been credited for bringing down the epidemic in formerly very high prevalence countries like Uganda40 and the introduction and scaling up of ART, just like male circumcision now, was received with some reservations. This is because of the fear that it could erode the gains achieved in controlling the spread of the epidemic. This study has shown that availability of ART has increased unsafe sex practices by encouraging people living with HIV/AIDS (PHAs) to sometimes suspend condom use, which was attributed to the desire to bear children by a previous study 41. Improvements in immunologic and clinical status and reduction in the risk of HIV transmission once ART is initiated could encourage PHAs on ART who wish to bear children to temporarily suspend condom use 42. This calls for an innovative approach to HIV prevention that addresses the childbearing desires of PHAs, especially in the context of discordance (one partner is HIV negative and the other is HIV positive). Experience in industrialized countries indicates that it is possible for ART to be overwhelmed by complacency about the threat of HIV/AIDS, leading to non-use of condoms. This could be attributed to the perception that HIV is now just another manageable chronic infection43; the perception that PHAs on ART are no longer infectious 44; the difficulty of adhering to a lifetime of condom use45; and the enhancement of quality of life and personal sense of well being which enables many PHAs to resume sexual activity. This change of sexual safety behaviour was noted in Kenya when Kemron and Pearl Omega drugs, introduced in the mid 1980s and 1993 respectively, were rumored to cure AIDS46. We therefore recommended that continuous HIV education and strengthening of other HIV prevention strategies including abstinence, faithfulness, and consistent use of condoms should accompany ART and any new HIV prevention methods, including male circumcision. Further research based on longitudinal studies is also needed to investigate male circumcision and condom use as the onset of non-use of condoms, if at all, is not known among newly circumcised males and their partners. Study limitations This study is limited by three main factors. Firstly, this was a cross-sectional study and therefore could not measure changes in condom use behaviour overtime. It is possible that those who circumcised later in life as in the present study, probably to reduce risk of infection with a sexually transmitted disease, could change their condom use behaviour in future. This requires a longitudinal study design to rule out HIV risk compensation after circumcision. Secondly, the study focused only on the last sexual intercourse and could therefore not assess consistency of condom use by circumcised males. Thirdly data on sexual behaviour and condom use are strongly affected by social desirability bias if respondents want to appear compliant with expected behaviours. The fact that these are also self reported could be a source of bias as well. Conclusion This study concludes that male circumcision did not impede condom use at the last sexual intercourse in Botswana. Non-use of condoms at the last sexual intercourse is impeded by religious beliefs, low level of education, marriage and stable unions, drunkenness, and misconceptions regarding ART as a cure of AIDS, or that ART reduces the risk of HIV infection. We recommended continuous HIV education and strengthening of the traditional ABC approach to HIV prevention to accompany ART and any new strategies including male circumcision. Acknowledgements The authors wish to acknowledge and thank the Central Statistics Office in the Ministry of Finance and Development Planning, Gaborone Botswana for allowing the authors to use the 2008 BAIS III data set. We also extend our thanks to the reviewers of this manuscript and all those who supported us in one way or another in writing this manuscript. References
Copyright © 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11111t4.jpg] [hs11111t2.jpg] [hs11111t3.jpg] [hs11111t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}