 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 11, No. 4, Dec, 2011, pp. 560-565 Social predictors of caesarean section births in Italy Kambale Mastaki J Independent Researcher, Via Leopardi,12/A, 60015 Falconara M, Italy Code Number: hs11112 Abstract Background: Caesarean section birth is a frequent mode of delivery worldwide. Several social factors have been demonstrated
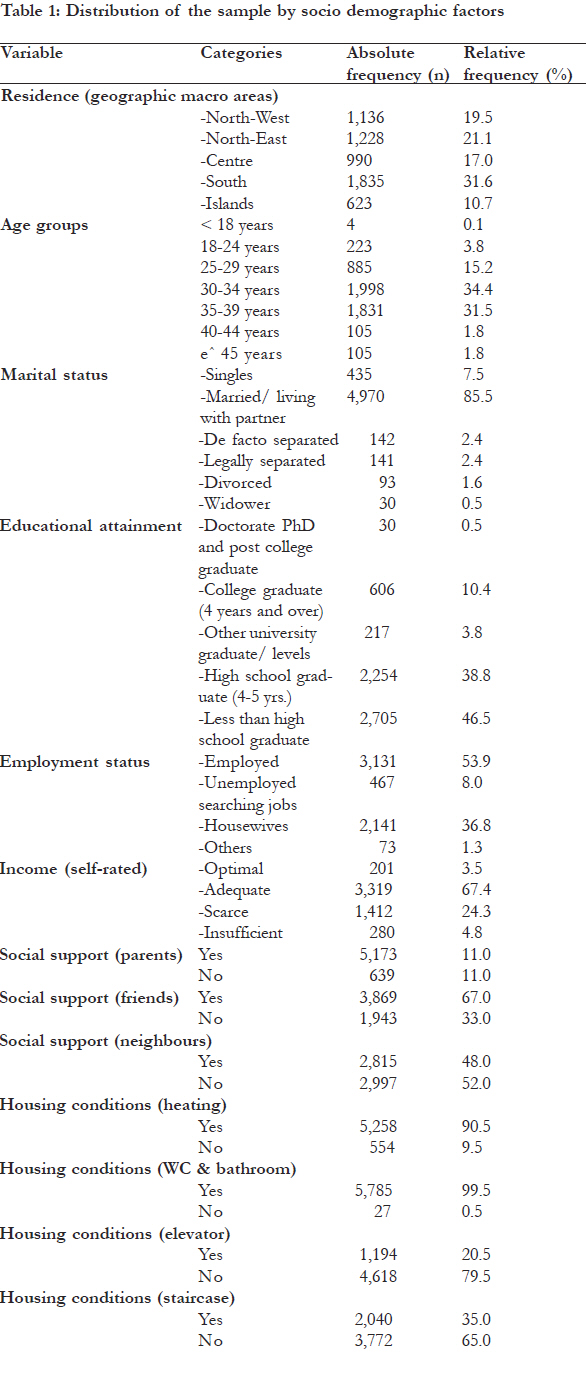
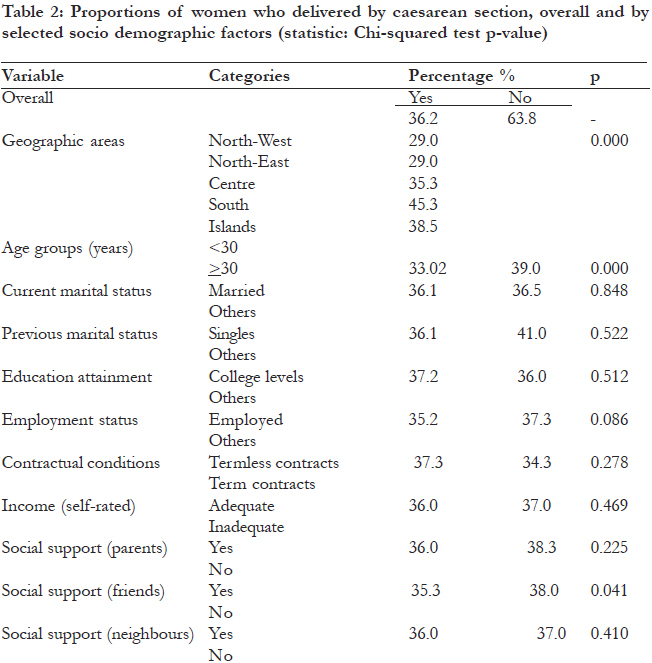
to be strong predictors of caesarean births. Keywords: caesarean births, social predictors, Italy. Introduction Caesarean section (CS) birth is a widespread mode of delivery worldwide in both developed and developing countries1-4. It probably is the most practiced surgical intervention in areas like sub-Saharan Africa 5,6. It can be performed in emergency context or on an elective basis and its main indications include previous caesarean section, labour dystocia or cephalopelvic disproportion, placenta previa or known vasa previa, conjoined twins, abdominal cerclage and abruptio placentae7. Several social factors have been demonstrated to predict delivery by CS. Race/ethnicity, age, educational attainment, employment, income and areas of residence have been investigated in relation to CS birth. Results frequently showed that positive predictors include black race 8,9, older ages9-11, some types of employment, and areas of residence12-15, lower educational attainment12,16 and high income15,17. This study intends investigate and update data about the social factors associated with CS birth in Italy, a developed country whose population is demographically characterized by a high rate of ageing population and a low birth rate18. Methods Design and tool Data for this study were drawn from the Italian National Institute of Statistics (ISTAT) survey conducted during the year 200519 . This is a quinquennial multipurpose population-based crosssectional survey with a complex design (stratified multistage random sampling). The 2005 survey comprised a nationally representative sample of 50,474 households (128,040 subjects). Inclusion criteria consisted of Italian women, resident in Italy, who delivered in the past five years prior to the survey and were not institutionalized at the moment of the survey. The following groups were excluded: immigrants, homeless subjects and, residents of rest homes, religious houses and penitentiaries. The 2005 ISTAT survey asked several questions about the delivery mode including whether (yes vs. no) the mother delivered by caesarean section. The comprehensive questionnaire (filled and administered by ISTAT professionals) used in the survey included socio demographics, healthcare, health and health-related factors. Variables As dependent variables, we used delivery mode (caesarean vs. vaginal) rates, while the explanatory variables consisted of all relevant available socio demographics, health factors, healthcare, and healthrelated behaviour (yes vs. no) and social support defined as availability of friends and/or neighbours in situations of needs (yes vs. no). Socioeconomic status was assessed by using age (cut-off: 30 years), educational attainment (college levels vs. others), employment status (employed vs. others), contractual conditions (term vs. termless contracts) and self-reported wealth using income as a proxy (optimal-adequate vs. scarce-inadequate). Residence, a 5-categories variable (five macro areas: Northwest, North-east, Centre, South and Islands), was included in models as dummy variables (reference: North-West). Statistical analysis Virtually all the variables of interest were systematically dichotomized by appropriate procedures in order to perform bivariate tests (TStudent t-test, Pearson chi-squared test). Multiple logistic regressions included binary and dummy variables. We first performed descriptive statistics. We then followed Student t-test and Pearson chisquared test in order to examine relationships between several variables and the caesarean births rate. We finally conducted multivariate analyses (multiple logistic regressions) in search of models which best fitted the data. Models included socio demographic factors adjusted for confounders (healthcare, health, health-related factors, and social support). Models’ fitting was based on the strategy of stepwise backward selection while the diagnosis was based on standard post logistic tests (pseudo-R2, post logistic Hosmer-Lemeshow test and ROC curve). All these analyses were carried out by the statistical package STATA 10.1/SE20 . Levels of statistical significance were set to 0.05. Results Socio demographics Our sample comprises 5,812 women (respondent women who delivered the past five years prior to the survey). South macro area shares the highest proportion (31.6%; n=1,835) of this population while the Islands have the lowest (10.7%; n=623). The centre macro area shares 17.0% (n=990) of this population [Table - 1]. The mean age of this population is 34 years (SD: 5.22). The bulk of this population group is concentrated in the age groups 4 (30-34 years; 34.4%) and 5 (35-39 years; 31.5%), 85.5% are married or living with the partner, 14.7 % is university/college graduated or has some college education, 54.0% is actually employed and 8% are unemployed searching for jobs and finally only 3.5% rated their income as being optimal [Table - 1]. Caesarean births Of these 5,812 respondent women, 2,102 delivered by caesarean section. Caesarean delivery rate was 36.2 percent overall [Table - 2]. Social factors which resulted associated to caesarean section in adjusted multivariate analysis were age (p=0.000) and residence (Reference: North-Western area; Centre: adjOR: 0.753, p=0.001; South: adjOR: 0.484, p=0.000; Islands: adjOR: 0.629, p=0.000) [Table - 3]. Discussion Overall, 36.2% (n=2,102) of the women from this sample delivered by caesarean section. This is substantially more than the WHO recommendations which stated that 15% shall be the expected maximum rate21 . Nevertheless, it is similar or slightly different from percentages reported in studies conducted in many other countries worldwide1-4. This diffused high rate of caesarean births is worrying especially since a large percentage has no clear medical indication22 . Problems of financial burden and significant morbidity can’t also be overlooked. Contrary to a precedent Italian study by Cesaroni23 , our study didn’t find an association between educational attainments (or several other socioeconomic predictors excepted for age and residence) and caesarean section birth rates. Geographical differentials North-South in socioeconomic factors, health and health behaviours is a well documented fact in Italy24 . Our findings are surprising as they show that living in the centre and southern macro areas and not in the affluent north has a protective effect against cesarean section births. However, similar results have also been documented in a previous Italian study conducted by Paparizzi et al.25 . Cultural factors (different attitude about on-request caesarean sections) and healthcare behaviors (different utilization of public and private services in various geographical areas) are probably the causes behind this singular fact. Extreme ages including older ones are constantly recorded as being at higher odds of caesarean section births. Reasons are numerous and include, among others, psychosocial (fear of losing the baby!) and medical factors (high risks of fibrous uterus or pregnancy-related health disorders)26 . In our study, age seems to have a protective effect against caesarean section. These odd results deserve further investigations. Important social factors like educational attainment, employment status, or income seem to have had a marginal role in the mentioned survey but problems of information bias cannot be ruled out. To sum up, data from our study show that age and residence are the relevant social predictors of caesarean section births in Italy. The limits of this study include the non specification of response rate, the non differentiation between repeated and first caesarean sections and “on request” caesarean sections from those performed following medical indications. Conclusion Caesarean delivery among Italian women is rather high (36.2%). Younger women and northern macro areas are categories at particularly high risks. References
Copyright © 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11112t1.jpg] [hs11112t3.jpg] [hs11112t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}