 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
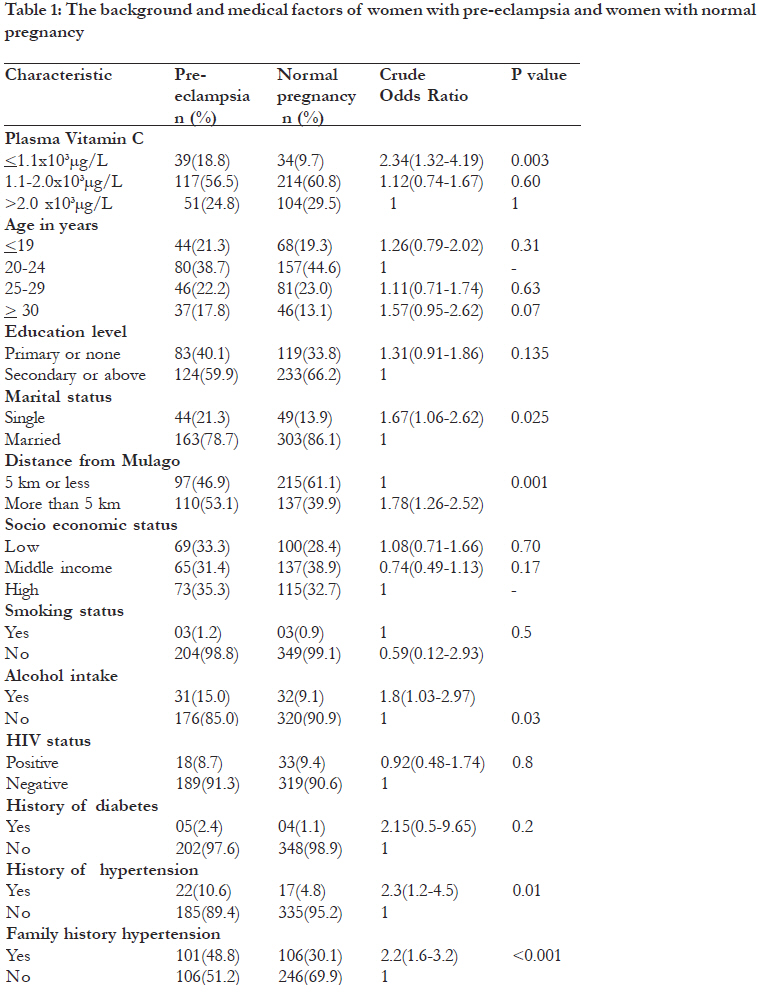
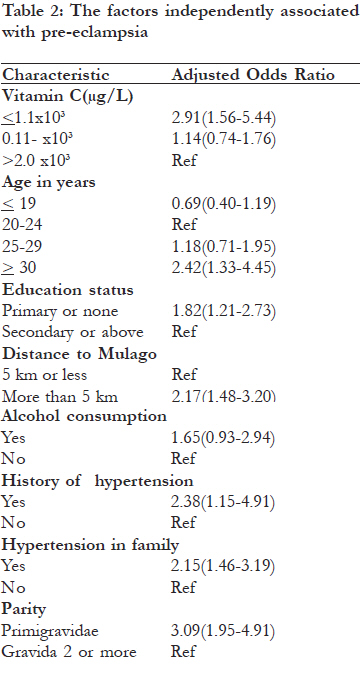
African Health Sciences, Vol. 11, No. 4, Dec, 2011, pp. 566-572 Plasma vitamin C concentration in pregnant women with preeclampsia in Mulago hospital, Kampala, Uganda *Kiondo P1, Welishe G2, Wandabwa J3, Wamuyu-Maina G4, Bimenya GS5, Okong P6 1 Department of Obstetrics and Gynaecology, Makerere University College of Health Sciences, Kampala, Uganda Code Number: hs11113 Abstract Background: Oxidative stress plays a role in the aetiology of pre-eclampsia and vitamin C may prevent pre-eclampsia. Key words: oxidative stress, pre-eclampsia, vitamin C Introduction Pre-eclampsia is a multi-system disorder in which hypertension and proteinuria develop in the second half of pregnancy. It affects 5-8% of first pregnancies although the incidence may be higher in low resource settings1. With other hypertensive disorders, pre-eclampsia is a leading cause of maternal, fetal, and neonatal morbidity and mortality world wide2, especially in developing countries where diagnosis and obstetric management are deficient. In a study by Kaye et al3 in Uganda, it contributed 17.6% of maternal morbidity and 21.4% of maternal deaths among women referred to the emergency obstetric unit. Despite extensive research on pre-eclampsia, its cause, prevention, and cure remain elusive. The management depends on early detection, use of antihypertensive treatment, seizure prophylaxis and delivery of the baby in severe cases4. This is the only way of preventing severe maternal morbidity and mortality although it increases the perinatal mortality because of premature delivery. Fetal survival depends on gestational age at delivery and is especially low in small-for-the-gestational age babies4. The placenta is necessary for pre-eclampsia to develop and there is reduced placental perfusion due to incomplete trophoblastic invasion of the spiral arteries5. These vessels remain muscular and this leads to reduced placental perfusion and ischaemia with production of superoxide through the xanthine/ xanthine oxidase pathway6. There is also an increase in the reduced nicotinamide dinucleotide phosphate (NADPH) oxidase activity which contributes to production of superoxide7. This leads to oxidative stress and a release of lipid peroxides, cytokines, and placental syncytiotrophoblast microvillous membranes from the placenta to maternal circulation which activate the endothelium8-9. The activated endothelium is responsible for the maternal syndrome in which there is hypertension, activation of microvascular coagulation, increased vascular permeability, proteinuria and altered vascular reactivity. There may be activation of platelets and leucocytes5. Oxidative stress exists when oxidants are in excess of antioxidants10 and it plays a role in aetiopathogenesis of pre-eclampsia. Vitamin C is a natural antioxidant, it is water soluble and is present in the diet. It protects poly unsaturated free fatty acids from oxidation by free radicals10. It also recycles oxidized vitamin E and glutathione which are important antioxidants. In the body there is a balance between oxidants and antioxidants10. In normal pregnancy there is an increase in both oxidants and antioxidants but the balance is maintained10-11. In preeclampsia there is a relative reduction in antioxidants and the plasma levels of vitamins C are reduced11-13. However, some researchers have not confirmed this finding14. Epidemiological studies show that vitamin C may play a role in the prevention and management of pre-eclampsia13,15. Although supplementation with vitamins C and E in pregnancy reduced oxidative stress, endothelial activation and preeclampsia16-17, this has not been confirmed by subsequent studies18-20. There is little information on the roles and function of vitamin C in pre-eclampsia in the Ugandan population. The major objective of this study was to determine the plasma vitamin C concentration and its association with pre-eclampsia at Mulago Hospital, Kampala. Methods Study design This case control study was conducted at Mulago Hospital from 1st May 2008 to 1st May 2009. Setting This study was conducted at Mulago hospital antenatal clinics. Mulago hospital is a National Referral Hospital for Uganda and a Teaching Hospital for Makerere University College of Health Sciences. It is also a District hospital for Kampala City Council. Women with complications in pregnancy in Kampala are referred to Mulago hospital for management. Study population The study population consisted of women who were attending antenatal clinics at Mulago hospital. Inclusion criteria Women were included in the study if they lived 15 kilometers or less from the hospital, were aged 1539 years with gestational ages of 20 weeks or more, and were willing to deliver at the hospital. Exclusion criteria Women were excluded if they had serious medical conditions like cardiac diseases or sickle cell disease. Sample size calculation The sample of 207 cases and 352 controls was obtained using a formula for case-control studies using OPENEPI software package21. We assumed the expected proportion of women in the lowest quartile of vitamin C level to be 53% as was found in a study by Zhang13, with 95% confidence interval, power of 80%, ratio of controls to cases of 2:1 and an odds ratio worth of detecting two. Definition of cases and controls Pre-eclampsia was defined as described in the classification approved by the International Society for the Study of Hypertension in Pregnancy22. A diagnosis of pre-eclampsia was made if a woman had hypertension and proteinuria after 20 weeks of gestation and previously had a normal blood pressure without proteinuria. The blood pressure resolved within six weeks after delivery. We checked the antenatal cards of the women to confirm the blood pressure and followed the women to the postnatal period. Women had hypertension if the blood pressure readings were 140/90mmHg four hours or more apart. The blood pressure was taken with a mercury sphygmomanometer, with a cuff 12cm wide, long enough to cover the upper arm after five minutes of rest, with a woman in a sitting position. The first Korotkoff sound was the systolic blood pressure and the fourth Korotkoff sound was the diastolic blood pressure. Significant proteinuria was defined as >300 mg protein in 24 hour urine collection or, if this was not available, 2+ proteinuria by dipstick on two consecutive occasions four hours or more apart. Urine samples were taken from the women who had hypertension for random protein measurement and then urine was collected for 24 hour protein determination. The control group was women with normal blood pressure after 20 weeks of gestation. Selection of cases and controls The cases were selected using computer generated random numbers until the sample size was attained. They were selected from the antenatal clinics by the research assistants who were trained midwives. After selection of a case two control women were selected using computer generated random numbers. Data collection The women were interviewed about their sociodemographic characteristics, medical and family history, and the present and past obstetric performances. In the socio demographic characteristics information was obtained about the age of the mother in completed years, the marital status, the level of education, and information of the mothers’ socio economic status. In the socio economic status information was obtained about the type of house the woman stayed in like the floor material, the wall material and the roofing material. Information was obtained about household properties like use of electricity, ownership of a fridge, television, radio, bicycle, motorcycle, vehicle, source of water, and the type of toilet facility. Each of these factors was given a score which was used as a proxy measure of the women’s socio economic status as described in the Uganda Demographic and Health Survey23. The women examined had a general and obstetric examination and, the blood pressure measurements were taken as described above. Blood was drawn at the time of recruitment for blood cell counts, renal and liver function tests, and vitamin C assays. For vitamin C assays, fresh blood was centrifuged within four hours to separate the plasma. The plasma was kept at -70oC until analysis. The assays were carried out in the Makerere University biochemistry analytical laboratory. Vitamin C was assayed using a colorimetric method as described by Kyaw24. This method determines ascorbic acid using acid phophotungastate. Briefly, 100μl of color reagent (acid phosphotungastate) was added slowly to 100μl of plasma in centrifuge tubes. The solution was mixed with a votex mixer and was allowed to stand for 30 minutes at room temperature. It was centrifuged at 3000rpm for 15 minutes. The blue-colored supernatant that formed was transferred to the Elisa plate- Multiscan Ex (Elisa Reader) Serial No: RS-232. The multiscan Ex is an eight channel light path filter photometer designed to perform standard photometric measurements. The absorbance at 620nm was read in pairs against a blank which was constituted with distilled water. Ethical considerations Ethical approval was obtained from the Mulago Hospital Ethics Committee, The Makerere University College of Health Sciences Ethics Committee and National Council for Science and Technology in Uganda. Written informed consent was obtained from the participants. The women below 18 years of age are emancipated minors and gave a written informed consent. Data analysis The data collected was checked, coded and double entered into Epi-Data 3.1 statistical software package. The data were cleaned and transferred to STATA version 10 and analyzed. The frequency distributions of the maternal socio demographic characteristics, medical and obstetric histories were examined and presented. Continuous variables like plasma vitamin C were checked and found to be approximately normally distributed. We plotted a qnorm plot in STATA and observed that the points were aligned in a straight line. In addition we plotted a histogram and found the bars to be aligned in a bell shaped curve. An independent t-test was used to find differences between means at 95% confidence level. A p-value of < 0.05 was taken as significant. Categorical variables were compared between groups using Chi-squared or Fischer’s exact test. To evaluate the association between preeclampsia and plasma vitamin C, a categorical variable was created from the distribution of the data since 72% of the women had deficient vitamin C, using 2.0 x 103μg/L as the cut off point25. Univariate analysis was done to assess the association of plasma vitamin C to the risk of preeclampsia. To adjust for confounding, variables which had a p-value of 0.1 or less at bivariate analysis, together with age were entered into a logistic regression model by a stepwise method. The factors in the socio-demographic characteristics were entered in the first model and adjusted. The factors that were significant from this model together with age were entered in the next model with medical factors and adjusted. The significant factors were entered in another model and adjusted against the obstetric factors. The factors which remained significant at this level were entered in a final logistic regression model with HIV and vitamin C levels and adjusted. The results are reported as odds ratios with the corresponding 95% confidence intervals. Results The baseline characteristics of the respondents are shown in [Table - 1]. The age of the women was 15-39 years with a mean of 25.1 (SD 5.86) years and a median of 24 years. About 64.6% of the women had acquired secondary educational level or above, 30.2% were of low socio economic status, 0.01% were smokers, 82.8% were married, 55.4% resided five kilometers or less from the hospital and, 11.2% consumed alcohol. However, women with pre-eclampsia were more likely to be single (p value <0.03), to stay further away from the hospital (p value <0.001) and were more likely to consume alcohol (p<0.03). The mean gestational age in weeks at which blood was drawn was 34.8 (SD 4.8) in the cases and 32.4 (SD5.8) in the controls. The mean plasma vitamin C in women with pre-eclampsia was 1.7 x 103 μg/L (SD=0.7), the range was 0.7-4.4x 103μg/L; and in women with normal pregnancy was 1.9 x 103 μg/L (SD=0.8); the range was 0.4-5.64x 103μg/L. The difference between the two means was statistically significant (p= 0.005). Seventy two percent of the women had deficient plasma vitamin C concentration using <2.0x103μg/ L as cut-off point. Women with pre-eclampsia were more likely to have low plasma vitamin C concentration (p<0.002). The association of plasma vitamin C levels with pre-eclampsia is shown in [Table - 2]. Women were categorized in three groups according to the vitamin C levels in plasma. After controlling for confounders, women who had low vitamin C concentration were 2.9 times more likely to develop pre-eclampsia compared to women with normal or high plasma vitamin C level. The confounding variables were: the age of the women, the education level, the marital status, the socio economic status, the distance from hospital, the parity, history of diabetes, history of hypertension and family history of hypertension, gestational age, HIV status, smoking, and alcohol consumption. Discussion This study investigated the plasma vitamin C concentration in women with pre-eclampsia and women with normal pregnancy. The mean plasma vitamin C concentration was lower in women with pre-eclampsia compared to that of women with normal pregnancy. This could be because women with pre-eclampsia have increased oxidative stress11. Vitamin C is the first line antioxidant defense in aqueous solution and is consumed during the oxidative process. A further reduction in vitamin C levels occurs as it recycles oxidized vitamin E and glutathione. These results are consistent with what was found by others11-13. Bowen et al11 found plasma vitamin C higher in pregnant women with normal blood pressure compared to women with pre-eclampsia. Similarly, Kharb12 reported plasma vitamin C to be significantly lower in women with preeclampsia compared to women with normal pregnancy. Zhang et al13 found the plasma vitamin C to be 18% lower in pre-eclampsia compared to women with normal pregnancy. However, the results from this study are in disagreement with what was found by others26-27. This could have been due to different methods of assay and lack of power in these studies. Robin et al26 studied 29 women with normal pregnancy and 21 women with pre-eclampsia, and Ozan et al27 studied 39 women with pre-eclampsia and 20 women with normal pregnancy. This could have accounted for the difference from our study because of smaller numbers. Most women in this study had deficient vitamin C. This is in contrast with what was found by Bowen et al11 in South African women and Kharb et al12 in Indian women. This could be due to the differences in the nutritional status of the women in these different communities. In this study women with low vitamin C levels were 2.9 times more likely to develop pre-eclampsia after controlling for confounders. This was similar to what was found by Zhang et al13 who found a 3.8 risk of pre-eclampsia in women who had low level of plasma vitamin C. They also found the mean dietary intake of vitamin C to be 13% lower in women with pre-eclampsia. The finding of low levels of plasma vitamin C in women with preeclampsia and the association of low levels of vitamin C with pre-eclampsia could imply that oxidative stress may play a role in the aetiology of pre-eclampsia5, although these results need to be corroborated with prospective studies. However, some researchers28 have taken samples from women at 13 weeks gestation. They have shown that women who develop pre-eclampsia on average have plasma vitamin C 10% lower than women who did not develop pre-eclampsia. In pre-eclampsia, there is inadequate trophoblastic invasion of the spiral arteries. This leads to placental ischaemia. The placenta releases factors into the maternal circulation which lead to endothelial dysfunction. There are antioxidants which counteract the effects of these oxidants and are consumed in the process. These include vitamin C, vitamin E and glutathione which are present in the extracellular compartment. The low levels of vitamin C in pre-eclampsia and the association of low level of vitamin C with the risk of pre-eclampsia shown in this study could imply that vitamins C may have a role in the management of pre-eclampsia. Some epidemiological studies13,15,29 show that high vitamin C intake is protective. Klemmensen et al15 in a population-based pregnancy cohort found a trend towards a protective effect for severe pre-eclampsia/ eclampsia in women with increasing intake of vitamin C. Bodnar et al29 showed that pre-eclampsia may be prevented through regular supplementation of multivitamins before conception. In fact vitamin C and E supplements given to pregnant women reduce oxidative stress and endothelial cell dysfunction17, and the occurrence of pre-eclampsia16. However, this has not been replicated in subsequent studies18-20,30. This could be due to the characteristics of the patients who were recruited, the time of initiation of treatment, and the fact that these studies were done in developed countries where the nutritional status of the women is high. It is likely that different results may be obtained if these studies are done in developing countries where the women’s nutritional status is low. Conclusion There was a strong association between low plasma vitamin C levels and pre-eclampsia in women attending antenatal clinics in Mulago Hospital, Kampala. Health workers need to educate pregnant women, especially women at risk, on nutrition and foods rich in vitamin C. This may improve their vitamin C status and reduce pre-eclampsia in Uganda and hence the maternal, fetal and neonatal morbidity and mortality associated with it. Acknowledgements We thank Makerere University and African Population and Health Centre for the support. References
Copyright © 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11113t2.jpg] [hs11113t1.jpg] |
| |||||||||

{kind=link}
{kind=link}