 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
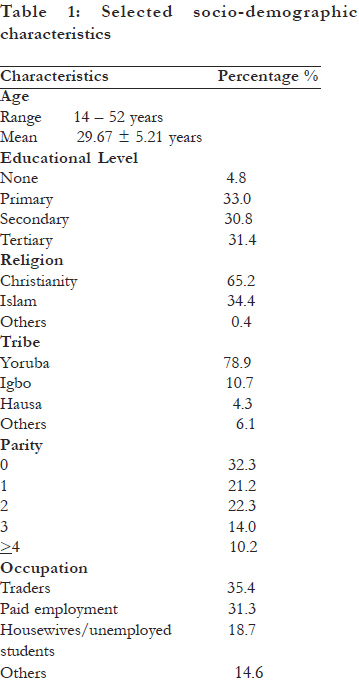
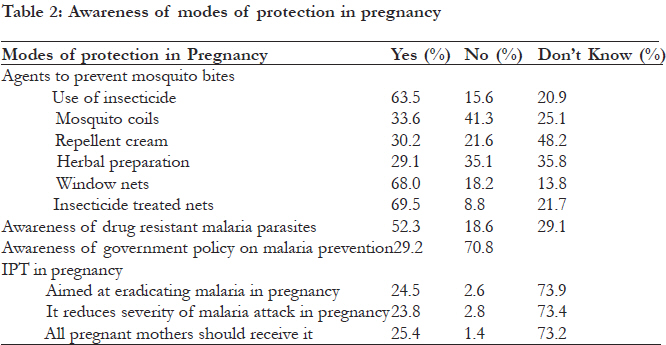
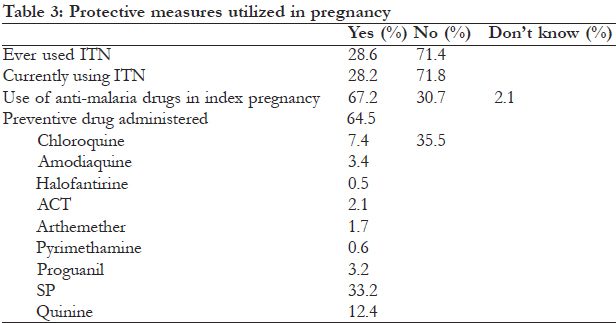
African Health Sciences, Vol. 11, No. 4, Dec, 2011, pp. 573-577 Knowledge and utilization of malaria control measures by pregnant and newly delivered mothers in Ibadan, Nigeria *Oladokun A1, Oladokun RE2, Adesina OA1 1 Department of Obstetrics and Gynaecology, University College Hospital, Ibadan, Nigeria Correspondence Address: Dr. A. Oladokun, Tel: 234 8033285279, email: sinaoladokun@yahoo.com, oladokun@comui.edu.ng Code Number: hs11114 Abstract Background: The World Health Organisation (WHO) guidelines for the control of malaria during pregnancy include prompt and effective case management of malaria combined with prevention of infection by insecticide-treated nets (ITNs) and intermittent preventive treatment in pregnancy (IPTp). Despite this the uptake is poor. Key words: malaria in pregnancy, chemoprophylaxis, intermittent preventive therapy Introduction Every year, approximately 50 million women living in malaria endemic areas become pregnant; half of them in sub-Saharan Africa, and many are in areas of intense plasmodium falciparum transmission1 (p.falciparium). In these regions, malaria in pregnancy is predominantly asymptomatic and yet it is a major cause of severe maternal anaemia and low birthweight babies2. Because of the strong association between low birth weight and child survival, successful control of malaria in pregnancy will not only save maternal lives but might also prevent 75 000–200 000 infant deaths every year3. It is thus of a high public health priority in all endemic countries. For sub-Saharan Africa (SSA), the WHO has developed guidelines for the control of malaria during pregnancy2. These consist of prompt and effective case management of malaria illness, combined with prevention of infection and/or disease by insecticide-treated nets and intermittent preventive treatment in pregnancy (IPTp).1,4 A recent systematic review has shown that insecticide treated nets (ITNs) are beneficial to both mother and newborn baby in SSA5. Indeed, it is one of the main strategies of the Roll Back Malaria (RBM) partnership. The ITNs, compared with no nets, substantially reduce the risk of placental malaria and adverse pregnancy outcome such as low birth weight (LBW) and stillbirth/ abortion.5 In addition, insecticide-treated nets that are provided to pregnant women have the added beneût that they continue to protect the newborn baby during infancy, since most babies sleep with their mothers.2 At the household level, in addition to ITNs, other protective measures include protective clothing, insect repellents and spraying of insecticides.6 In sub-Saharan Africa, until the mid to late 1990s, prevention of malaria in pregnancy relied on weekly chloroquine prophylaxis.2 This mode of prevention, however, had the challenge of poor compliance.7 Intermittent preventive treatment in pregnancy was explored and developed to avoid the limitations of daily or weekly chemoprophylaxis.8,9 It consists of an antimalarial treatment given at regular intervals during pregnancy, regardless of malaria infection or disease. In areas of stable P. falciparum transmission, WHO recommends Sulphadoxine-Pyrimethamine (SP) combination on account of it being cheap, easy to administer (single dose), and safe in the second and third trimester. At least two doses are given from the second trimester onwards at least one month apart. 1 It was initially thought that a drug regimen based on a few supervised doses would overcome the compliance limitations of chemoprophylaxis. In addition, concomitant insecticide-treated net use might reduce the need or frequency of IPTp dosing. However, studies in countries where IPTp has been implemented for several years show that the uptake of a second dose is surprisingly poor. 1, 10 More operational research is needed to develop strategies to improve the uptake and effectiveness of this promising strategy. The aim of the study was to assess the level of adherence to the Intermittent preventive treatment in pregnancy (IPTp) using the Sulphadoxine-Pyrimethamine (SP) combination as recommended for the pregnant mothers. Methods The study was a cross-sectional survey of 1330 consented pregnant and newly delivered mothers in one hundred and thirty-two (132) hospitals and maternity centres in Ibadan metropolis over a period of one year from April 2008 to April 2009. Ethical approval for the study was obtained from the University of Ibadan/University College Hospital (UI/UCH) Health Research Ethics Committee (UI/IRC/07/0111) A list of the registered government and private hospitals within Ibadan metropolis was obtained from the State Ministry of Health which contained the 132 hospitals and maternity centres. All the hospitals and maternity centres were sampled. An average of 10 consecutively consented (written) pregnant and newly delivered mothers who were in the hospitals and the maternity centres at the time of visit were recruited into the study. Information obtained on the knowledge and utilization of malaria control and treatment in pregnancy after obtaining their consent was entered into Microsoft excel file and analysis done using SPSS 16 software package. Results are presented as frequency tables. Results During study period, 1330 pregnant and newly delivered women in 132 facilities within the Ibadan metropolis were surveyed. The mean age of the respondents was 29. 67 years (±5.21). Over sixty percent (62. 2%) of the women had had 6 or more years of formal education. Most of the women were Christians (65.2%), and of Yoruba tribe (78.9%). The primigravidae was the commonest parity reported. Slightly over one-third of the respondents were traders. [Table - 1] The modes of prevention most commonly reported as being effective for the prevention of malaria in pregnancy were the use of insecticide spray, window nets and ITNs. While about half of the respondents were aware of the concept of drug resistant parasites, less than one-third (29.2%) of the respondents were aware of a new government policy on the prevention of malaria in pregnancy. [Table - 2] While only 28.6% of the respondents had ever used ITNs and a similar proportion (28.2%) were using ITNs in the index pregnancy, about two-thirds (67.2%) of the women had had a drug administered for prophylactic purposes in the index pregnancy. Of the patients who had had preventive drugs administered the commonest drug prescribed was the SP combination. In response to the question asking if the respondent had received treatment on account of malaria in the index pregnancy only 1,041 (78.3%) responded. Of this only 48.8% (508) responded in the affirmative about having received malaria treatment in the index pregnancy. [Table - 3] Discussion This study shows a disturbing gap between knowledge and practice. Although most of the women were aware of the protective nature of ITNs, it was observed that very few of them were actually using these ITNs. This finding is consistent with other reports from south-west Nigeria which showed that the majority of the people used screens and sprays to protect against malaria while the use of ITNs was poor.6,11 It has been proposed that since the cost of the net is often not affordable by the group particularly vulnerable to malaria and its deleterious effects i.e. very young children and pregnant women, it may be ideal for the Federal Government of Nigeria to make ITNs available at a highly subsidized rate6. In contrast to the poor usage rate of ITN, a large proportion of parturient women in this study received prophylactic drugs for malaria but disturbingly, over half of the drugs were not those currently recommended by the WHO or the Federal Ministry of Health i.e. sulphadoxine-pyrimethamine. This is in spite of the fact that Nigeria adopted the IPT strategy in year 200512, 13. The WHO expects 80% of all pregnant women living in areas of high transmission to receive IPTp during pregnancy by 201014. However, the coverage of the intervention is still low. A similar scenario was seen in Kenya, one of the first countries to implement IPTp. Its national coverage for two doses of SP was only 4% five years after IPTp implementation13, 15. Various reasons have been proffered for the poor adherence to this simple regimen. These reasons could be patient or health worker related13. In two Tanzanian studies, low compliance with the use of SP was partly attributed to health care providers’ and users’ fear of side effects of SP and their inadequate knowledge of the correct dose. Most respondents were said to have believed that antimalarial drug when taken during pregnancy could be harmful to the pregnant women and the unborn children16. The most commonly prescribed drugs for treatment as reported by the women were chloroquine and SP. Again, this is in spite of the current National Malaria Treatment Guideline and Policy in Nigeria that recommends quinine for treatment of clinical malaria in all trimesters12. Artemisinin based combination therapy (ACT) is recommended as second line agents in the second and third trimesters and may be used in the first trimester where there are no suitable alternatives12, 13,17. Quinine and ACTs did not feature prominently in the drugs reported by these women for treatment. This study demonstrates awareness of vector control measures but poor use of these measures by these pregnant women. In addition, there is poor use of the recommended agent for IPTp. While the factors militating against the use of these preventive measures need to be urgently explored and addressed, the national malaria control unit through the health facilities may have to provide ITNs and SP free of charge. Conclusion The government not only needs to educate the public in general and pregnant women in particular on the current approach to the prevention and management of malaria in pregnancy but plausible interventions to address the gaps and deficiencies must be developed. All of these will contribute to the attainment of the MDGs of improving the health of mothers and new-borns. Acknowledgement This study received support from the Senate Research Grant of the University of Ibadan, Nigeria. References
Copyright © 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11114t3.jpg] [hs11114t2.jpg] [hs11114t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}