 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
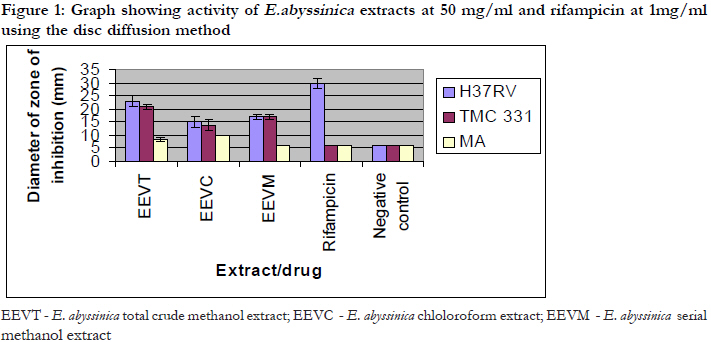
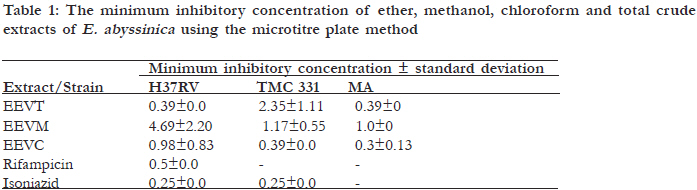
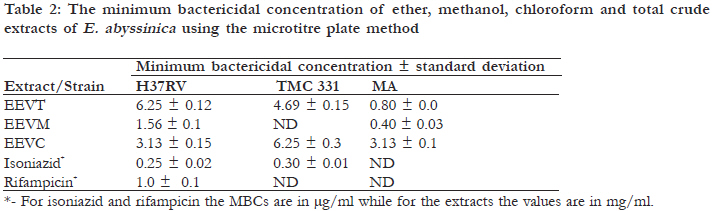
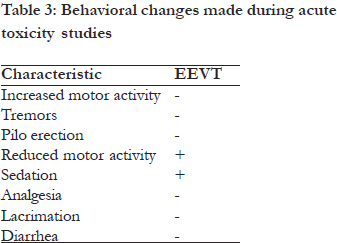
African Health Sciences, Vol. 11, No. 4, Dec, 2011, pp. 587 – 593 The efficacy of the crude root bark extracts of Erythrina abyssinica on Rifampicin Resistant Mycobacterium tuberculosis Bunalema L1, * Kirimuhuzya C1, Tabuti JRS2, Waako P1, Magadula JJ3 , Otieno N3, Orodho JA4, Okemo P5 1 Department of Pharmacology and Therapeutics, Makerere University College for Health Sciences Code Number: hs11116 Abstract Introduction: Tuberculosis (TB) is one of the leading causes of morbidity and mortality with a global mortality rate at two million deaths per year while one third of the world’s population is infected with the TB bacillus. Key words: Erythrina abbyssinica; Mycobacterium tuberculosis; rifampicin-resistance Introduction Tuberculosis (TB) is one of the leading causes of morbidity and mortality globally. The global mortality rate stands at two million deaths per year with one third of the world’s population infected with the bacillius1, 2, 3. It is estimated that 9.2 million new cases are diagnosed every year. According to the World Health Organization (WHO), the incidence of tuberculosis in African countries more than doubled between 1990 and 2005 and is taking an upward trend3. Africa carries 29% of the world’s disease burden and 34% of the world’s total death rate4. The world is currently beleaguered with multi drug resistant (MDR) as well as extensively drug resistant TB (XDR) forms of Mycobacterium tuberculosis (MTB) which are threatening to make both the first and second line drugs useless1,5, 6. The situation is made worse by co-infection with HIV among patients. Autopsy studies have shown that 50% of the 40 million HIV-infected individuals die from TB7. Treatment of TB patients co-infected with HIV/ AIDS has been associated with treatment failure, relapses, and acquired drug resistance in addition to drug interactions that increase the risk of toxicity8,9. There is, therefore, need to develop new, more effective, and safer anti TB drugs. Natural products can provide new and important leads in the drug discovery process10. In 2007, an ethno botanical survey to identify plants used to treat tuberculosis in the Lake Victoria basin was carried out and traditional practitioners who claimed to treat TB were reportedly using a number of medicinal plant species19. However, the efficacy and safety of these plants against Mycobacterium tuberculosis was one of them had not been scientifically validated. This study therefore was designed to investigate the effectiveness and toxicity of crude extracts of Erythrina abyssinica Lam. ex DC [Family: Fabaceae] against various strains of Mycobacterium. E. abyssinica has a taxon range throughout East Africa and may grow as a scattered tree in wooded grassland or in open deciduous woodland or on rocky hillsides. It can also be grown as a ‘living fence’ from truncheons12. Methods Study design This study was conducted using an experimental design. The root bark of Erythrina abbyssinica (Ejirikiti in Luganda) was collected from Mukono district, at an altitude of 1,220 metres above sea level at 00°20’N 32°44’E, and crude extracts prepared and tested in a bioassay on three strains of mycobacteria. Susceptibility tests, MIC and MBC for the active extracts were carried out. Phytochemical screenings, as well as acute toxicity tests, for the most active extracts were also performed. Selection criteria The study plant was selected basing on the fact it had been mentioned by at least three traditional healers as being used in the treatment of symptoms of TB and that it had never been worked on for antimycobacterial activity in Uganda. Plant collection and identification The root bark of E. abbyssinica was harvested and the collected specimens were identified at the Department of Botany, Makerere University. Voucher specimen (JRST 784) was prepared and kept at the Makerere University Herbarium. Drying and pulverizing The plant parts were dried under shade, to avoid direct sunshine that could degrade some of the compounds in the plants. They were also turned over regularly, to avoid fermenting and rotting. The dried parts were then pulverized using a plant mill, the powder weighed using an analytical scale, and stored at room temperature. Extract preparation A total crude methanol extract was prepared by soaking 500 g of the powder in 1000 ml of methanol for seven days. Then another 500 g plant powder was serially extracted by soaking in 1,000 ml of ether, chloroform, and lastly methanol, following the order of polarity of the solvents, for three days each, with occasional shaking. Whatman’s filter paper No.1 was used for filtering to obtain the crude extract solution. The crude solution was then concentrated to a minimum volume by a rotary evaporator (Büchi Labortechnik AG, Switzerland) at 40°c and reduced pressure. The concentrated crude extracts were then allowed to evaporate to constant weight at room temperature. Mycobacterial tests These tests were done in a level three-safety laboratory at the Joint Clinical Research Center (JCRC) in Mengo, Kampala, Uganda. Mycobacterium strains used Three preserved strains of Mycobacterium used were obtained from the Joint Clinical Research Centre (JCRC) at Mengo in Kampala. They included a rifampicin-resistant strain (TMC -331strain) to serve as an indicator of MDR, a fully susceptible strain (H37Rv) as a control, and Mycobacterium avium (MA), a wild strain from a Ugandan patient to represent the Mycobacterium other than tuberculosis (MOTT) group. Growth media Middle brook 7H10 agar supplemented with oleic acid-albumin- catalase (OADC) was used for reviving and culturing the mycobacteria for sensitivity testing. The medium was from Becton Dickinson Microbiology Systems of Becton Dickinson Company (DifcoTM), 7 Loveton Circle, Sparks, Maryland, USA; Lot No. 8175150.The OADC, Lot 8136781, also from Becton Dickinson Company. No adjustments for pH were made. Preparation of inoculum for drug sensitivity testing Preserved strains were revived on Middle brook 7H10 agar, prior to anti tubercular susceptibility testing. Colonies were scraped from freshly growing colonies (three weeks old) on Middle brook 7H10 plates and introduced into 10ml of saline. Bacterial suspensions with 0.5 McFarland standard turbidity equivalents to 108 CFU were prepared by dilution with saline. The tubes were vigorously vortexed for 30 seconds in a glass bottle containing glass beads and the particles allowed to settle13. Bioassay protocol for susceptibility tests Preparation of the drugs/ extracts The dried crude extracts (1 g) were each dissolved in methanol (20 ml) to a concentration of 50 mg/ ml. Sterilization of the extracts was done using 0.2μm single use filters. For rifampicin, a stock solution of 5.0 mg/ml was prepared by dissolving 0.1g in 10 ml of methanol. A stock solution of 2.5 mg/ml of isoniazid was prepared by dissolving 0.1 g in 20 ml of distilled water. Preparation of biodiscs A volume of 20μl for each of the drugs and extracts was used per disc, for the general susceptibility tests so that for the extracts each disc contained 1mg of the extract; 0.05mg/disc of isoniazid and 0.1mg/ disc for rifampicin. The discs were left to dry for 24 hours. The culture medium was sterile Middle brook 7H10 agar placed in 90 mm diameter Petri dishes with quadrants. In each quadrant of the Petri dish was put 5.0 ml of the medium. The solidified medium in the quadrants was inoculated using a swab. A rifampicin impregnated disc was placed in the first quadrant, in the second quadrant was put an isoniazid impregnated disc the third quadrant had an extract impregnated disc while the fourth quadrant contained a blank disc as a negative control. All the tests for the extracts and the three strains of Mycobacterium were done in triplicate. The Petri dishes were then left in the hood overnight, to allow diffusion of the extracts and drug and then sealed with a carbon dioxide-permeable tape. These were then incubated at 37°C in a carbon dioxide incubator for up to four weeks. The sensitivity of M. tuberculosis and M avium to the extracts and the drug was determined by measuring the zones of inhibition surrounding the disc using a millimeter scale. Determination of the Minimum Inhibitory Concentration (MIC) Microtitre plate method was used in the determination of MIC. Serial dilutions of the drugs /extracts were used to determine the minimum inhibitory concentration of the drug or extract, using Middle brook 7H9 from Becton Dickinson Microbiology Systems of Becton Dickinson Company (DifcoTM), 7 Loveton Circle, Sparks, Maryland, USA; Lot No. 5123072 as the medium. The OADC, Lot 8136781 was also from Becton Dickinson Company14,15. No adjustments for pH were made. Procedure The procedure followed was that described by Pauli et al13, with some modifications. Middle brook 7H9 broth (100 μl) was dispensed into all the wells of a sterile 96-well microtitre plate. Then 100 μl of each of the drugs and extracts was added using a pipette. The drug/extract was mixed well with the medium, by sucking up and down six times and then serial doubling of dilution was made. This was done by successive transfers of 100 μl up to column 10, with the 100 ìl from the well in column10 being discarded instead of placing it into column 11. With a pipette, 5 ìl of bacteria (104-105 CFU/ml) were dispensed in columns 1 to 11 for all the rows containing the drugs and extract. The well in column 12 was left blank, as a sterility control. The solvent used to dissolve the drugs was also titrated in one of the rows as a control for solvent. All the MIC tests were done in duplicate and the plates were then incubated at 37°C for up to four weeks. The lowest concentration with no visible turbidity was taken to be the MIC. Minimum bactericidal concentration This was done by sub culturing ten-fold dilutions of the contents of the wells that showed no apparent growth in the MIC test. The dilution was made by pipetting 10μl of the contents of each of the wells diluting it to 100 μl with fresh Middle brook 7H9 broth. Incubation was then done for up to six weeks. The minimum concentration in the MIC test that produced no growth after the ten-fold dilution was taken to be the MBC. Acute toxicity tests Acute toxicity tests on the most active extract were carried out on mice, Mus musculus. It was done as described by Ghosh16 , but with few modifications. Only the total crude was tested. Mice of both sexes, for each concentration were used and they were fasted overnight before giving them the extracts orally using a gastro intestinal tube. A pilot study was carried out on pairs of mice, using widely separated doses of 50,200,500, 800 and 1000 mg/kg to determine approximate lethal and non-lethal dose ranges. Five different groups of five mice each were used in the experiment given in doses of 700,750, 800, 850 and 900 mg/kg body weight as a single dose. The control groups were given DMSO. Observations were made and recorded after 24 hours. The LD50 was then determined by plotting percentage mortality against log dose graph. Qualitative phytochemical testing In the most active extracts qualitative tests for terpenoids, saponins, tannins, flavones, phenols, and alkaloids were carried out as described by Edeoga et al17. Test for terpenoids To the extract (1ml) chloroform was added and then an equal volume of conc sulphuric acid was added. Formation of a bluish red coloration indicated presence of terpenoids. Test for tannins The dried powdered extract (0.5g) was boiled with water (20ml) in a test tube and then filtered. Few drops of 0.1 M iron III chloride (FeCl3) solution were added. Formation of a blue-black coloration indicated presence of tannins. Test for flavones Ammonium solution (5ml) was added to a portion of aqueous filtrate of the extract followed by addition of sulphuric acid. A yellow coloration indicated presence of flavones. Test for phenols Iron III chloride (2ml) was added to the extract (2ml). Formation of a deep bluish solution indicated presence of phenols. Test for alkaloids About 50g of the powder was mixed with 250ml of 1% sulphuric acid. It was allowed to stand and then filtered. 10mls of the filtrate was shaken and added t Meyer’s regent. Formation of a white precipitate indicated presence of alkaloids. Results Antimycobacterial activity The powdered sample was boiled in distilled water (20ml) and filtered. The filtrate (10ml) was mixed with distilled water (5ml) and shaken vigorously. Formation of a persistent froth indicated presence of saponins. Data collection and analysis The numerical data from the replicated investigations is presented in form of tables and histograms. Statistical analysis involved use of the statistics computer program, SigmaPlot, New Version 10, of Systat Software Inc. (2002) and Graph pad prism version 5. Ethical considerations Ethical approval was sought from the Research and Ethics Committee of the Makerere University college of Health Sciences and the Uganda National Council for Science and Technology. Protection of the investigators was ensured by carrying out the work in collaboration with, and under the guidance of the mycobacteriology laboratory staff at the Joint Clinical Research Centre, Mengo in Kampala, who had the necessary knowledge for handling M. tuberculosis. Also the necessary protective wears including respirators and gloves as well as safety cabinets were used, to minimize the risk of exposure to M. tuberculosis. Guidelines for the handling of laboratory animals were followed. Animals were sacrificed under general anesthesia16. [Figure - 1] The susceptibility tests were done in triplicate and the mean of the three values and standard deviation are presented in [Table - 1]. The zones of inhibition also include the diameter of the disc which is 6mm. Rifampicin was not active on Mycobacterium avium complex and a rifampicin resistant strain TMC- 331 but it showed a zone of inhibition of 26 mm for H37Rv (a pan sensitive strain) at a concentration of 0.1 mg. Isoniazid cleared the quadrant for two strains at a concentration of 0.05 mg/ml. E. abyssinica total crude methanol extract showed the highest activity on the pan sensitive starin H37Rv (0.39±0.0mg/ml) and the rifampicin-resistant starin, TMC-331, 2.35±1.11g/ml) and was also activive on Mycobacterium avium (0.39±0.0mg/ml). The negative control showed no activity as indicated in [Table - 1]. Minimum inhibitory concentration of E. Abyssinica From [Table - 1] the chloroform extract from E. abyssinica had the lowest MIC value against both Mycobacterium avium wild strain and the rifampicin resistant strain followed by the methanol extract while its total crude extract had the lowest value against H37Rv, followed by the chloroform extract. Minimum bactericidal concentrations The MBC values for total crude methanol extract were 6.25, 4.69 and 0.80 mg/ml for H37Rv, TM-331 and M. avium, respectively while the corresponding values chloroform extract were 1.56, 6.25 and 0.40 mg/ml, respectively. For the serial methanol extract the MBC values were 3.13, 6.25 and 3.13 mg/ml respectively while the serial ether extract showed no activity at concentrations used while for rifampicin which was active only on H37Rv, the value was 0.5μg/ml. Isoniazid had its MBC values for H37Rv and TMC- 331 as 0.25 and 0.5μg/ml for both H37Rv and TMC- 331. [Table - 2] Results of acute toxicity tests [Table - 3] shows behavioral changes that were made during the first six hours after drug administration. The behavioral changes that were observed during the first six hours after the mice were administered with E. abyssinica total crude extract included decreased motility, sedation,frequent urination and finally tremors. The control group was given DMSO and no peculiar changes in behavior were observed. A single dose administration of E. abyssinica total crude extract, no death of mice was recorded within the first six hours of drug administration. The doses that were given were estimated from a preliminary study. From a plot of the percentage mortality of mice against log dose administered and analysed using Graphpad, LD50 of E. abyssinica crude extract was found to correspond to a log dose of 2.99, which corresponds to 776.2mg/ kg body weight. Discussion From the study the methanol total crude, serial chloroform and methanol extracts of E. abyssinica showed activity against all the three strains used. Against the pan sensitive strain H37Rv, total crude extract of E. abyssinica showed the highest activity followed by its chloroform extract. The potency of the extracts as compared to the standard drugs used was still very low. This is understandable considering the fact isoniazid and rifampicin we were comparing the activity of crude extracts with that of pure compounds known to be the most active against M. tuberculosis. If the active compounds could be isolated and purified, it is possible that they could show a comparable activity or even more activity than some of the drugs currently in use. A case in point is the activity shown by the crude extract against the rifampicin-resistant strain of MTB and M. avium to which rifampicin was clearly ineffective. There is a possibility that these extracts could also be active on some MDR TB strains since rifampicin is a good indicator of multi drug resistant TB. The chloroform extract of E. abyssinica was most active on TMC-331 and its high activity may be attributed to the presence of terpenoids. Phytochemical tests on the extracts showed presence of alkaloids, terpenoids, saponins, tannins and flavones. The total crude extract of E. abyssinica contained all the compounds while the methanol extract contained alkaloids, terpenoids and flavones. This could be the possible explanation for the high activity of the E. abyssinica extracts on mycobacteria. The chloroform extract of E. abyssinica contained only terpenoids, which could explain why the extract was most active on M. avium and the rifampicin resistant strain. According to Copp18, secondary metabolites of terpenoid origin lead the number of natural products with reported antimycobacterial activity due to their lipophilic nature and therefore ability to penetrate the mycobacterial wall. The results of antimycobacterial activity of E. abyssinica are comparable to findings on E. indica, a species from the same genus by Waffo et al17. In their study E. Indica showed antimycobacterial activity against E. smegmatis and Indicanine B, an isoflavonoid was reported to be responsible for the activity. Further studies are, however, needed to isolate and identify the antimycobacterial compounds in E. abyssinica. Acute toxicity studies carried out on the total crude extracts of E. abyssinica revealed that the extract had an LD50 of above 500mg/kg body weight which according to Gosh14, is considered to be relatively safe. Behavioral changes that were made included sedation and decreased motor activity at doses higher than 500 mg/kg body weight. The observations could have been central nervous system (CNS)-related. The results of this study have further shown that the search for new bioactive products using the ethno botanical criterion increases chances of finding active compounds which could be leads for new drug development against TB20. However, for E. abyssinica not many studies have been done concerning its toxicity and therefore, more studies are needed before declaring it to be safe for use. Study limitations The results from acute toxicity tests have shortcomings in that they measure mortality and sub lethal toxicity. Also, the tests measure only acute toxicity produced by a single dose, and not longterm toxicity and therefore, cannot measure idiosyncratic reactions though such reactions may be more relevant in practice than high dose toxicity. There were also problems associated with dissolving the crude extracts because they contain both the polar and non-polar compounds. A repeat of the tests after isolation and purification of the active compounds is likely to give variations in the results. Conclusion The results of this study have revealed that E. abyssinica has reasonable antimycobacterial activity, notably against rifampicin-resistant tuberculosis, and is relatively safe for use in as far as lethality is concerned. This therefore validates its use in the treatment of tuberculosis by traditional practitioners. However more studies on the toxicity of the plant are needed before declaring it completely safe for use in humans. Recommendations The active compounds of the plants should be isolated and identified. It is also recommended that, some tests be done to find out whether these compounds could have a synergistic effect on each other and also whether they are active on the resistant strains of TB. Further research on the toxicity of E. abyssinica should be ventured into to get a complete toxicity profile of the plant. Acknowledgements We would like to acknowledge Lake Victoria Research Initiative (VicRes) which gave financial support to the project; Uganda National Council for Science and Technology who gave permission to conduct the research; Makerere University, Departments of Pharmacology and Therapeutics and of Botany who provided logistics; the staff of the Mycobacteriology Laboratory of the Joint clinical research Centre (JCRC) , Mengo, Kampala, where the TB work was done; the healers who provided information and the research assistants who participated in colleting data. References
Copyright © 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11116f1.jpg] [hs11116t3.jpg] [hs11116t1.jpg] [hs11116t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}