 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
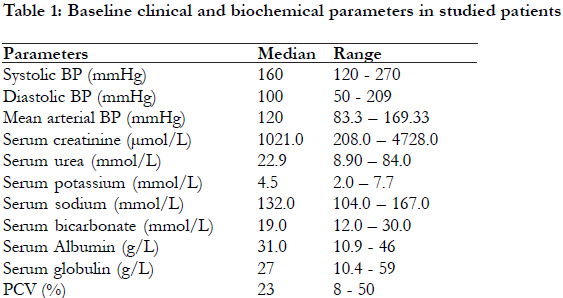
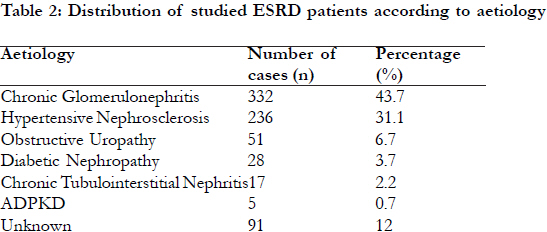
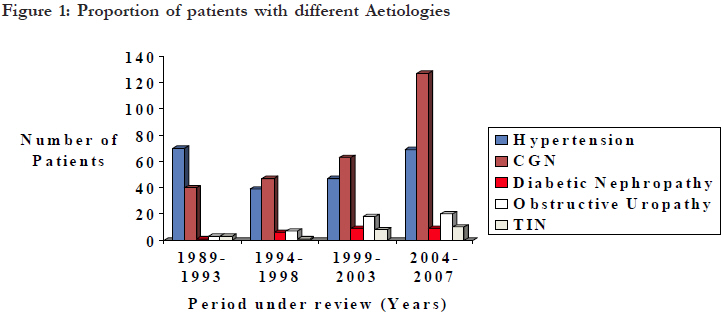
African Health Sciences, Vol. 11, No. 4, Dec, 2011, pp. 594 - 601 The pattern, clinical characteristics and outcome of ESRD in Ile-Ife, Nigeria: Is there a change in trend? *Arogundade FA, Sanusi AA, Hassan MO, Akinsola A Department of Medicine, Obafemi Awolowo University / Teaching Hospitals Complex, P.M.B 5538 Ile-Ife, Osun State, Nigeria Code Number: hs11117 Abstract Background: The prevalence of chronic renal failure and End Stage Renal Disease (ESRD) has remained high worldwide and the epidemiology has changed significantly in the last decade in industrialised countries. While there have been significant improvements in these patient’s outcomes in developed countries, their state and survival is still appalling in developing countries. Key Words: ESRD, dialysis, survival. Introduction Chronic kidney disease (CKD) and end stage renal disease (ESRD) are highly prevalent in both industrialized and developing countries of the world and the epidemiology has changed remarkably in the last decade particularly in the developed countries with diabetic nephropathy now assuming epidemic proportions1-6. While most industrialised countries have developed efficient renal registries, its either none existent or at its infancy in most developing ones hence only hospital derived data are available for planning. In addition, while major developments have occurred in the management of ESRD patients worldwide with significant improvements in outcomes, their clinical state and survival is still very poor in developing countries where GDP per capita is low and budgetary allocation on health is poor 1,2,4. The epidemiology of ESRD is strikingly different in sub Saharan Africa (SSA) compared with developed economies. While it predominantly affects the middle aged and elderly populations in developed countries, it picks out the young adults in their prime of life and the most economically productive years in SSA2,4,7-13. This may be attributable to the probable aetiology of CKD in the sub-region, and other factors that may contribute include poor access to care, poor knowledge of risk factors for CKD as well as deleterious socio-cultural practices. Diabetes Mellitus has emerged as the commonest cause of ESRD in developed countries followed by hypertension but it ranked a distant third amongst causes of ESRD in SSA with CGN and HTN being more prevalent. An earlier report on the causes of chronic renal failure (CRF) from our centre identified CGN and hypertension as the commonest causes while diabetic nephropathy (DN) was not reported at all among the causes of CRF9. Several other reports in Nigeria and other countries in SSA have established that HTN and CGN are the leading causes of ESRD, but the prevalence of diabetic nephropathy is rising and obstructive uropathy and toxic nephropathies also contribute significantly10-15. The outcome of ESRD in SSA is very poor and this is principally as a result of poor awareness of kidney disease in the community, late presentation to the hospital, limited capacity of health workers in kidney disease prevention and limited accessibility as well as affordability of renal replacement therapy (RRT) 16-18. In fact in a recent publication by Grassman et al19, Africa contributed less than 5% of patients on RRT worldwide. As a consequence of these, preventive nephrology strategies would be most beneficial in the sub-region and everyone should participate including governments and nongovernmental organisations 2. However to be able to plan a useful CKD prevention program in any community, there would be a need for background statistics on possible magnitude of CKD, probable predisposing factors or causes and mode of presentation. In this short report we sought to determine epidemiology of ESRD, modes of presentation as well as determine the major causes of ESRD. This we believe is vital and useful in planning prevention program in our community which would be representative of most communities in SSA. Methods Our hospital is a tertiary referral hospital based in south-western Nigeria and it served a population of above 15 million people in six contiguous states until the recent proliferation of renal care centres. We also have few referrals from eastern and northern states. Access to renal care is limited to major cities in Nigeria and renal replacement therapy is borne directly by the patients. The case records of all patients with chronic renal failure (CRF) managed during the 19 year period (1989-2007) was retrieved. The data on major causes, clinical presentation, renal replacement therapy offered and survival were retrieved and collated. The CRF was defined as presence of persisting and progressive deterioration in renal function manifesting as recurrent features of uraemia, oedema and/or hypertension persisting for longer than three months and supported by renal ultrasonographic evidence of either reduced kidney size or cystic or hydronephrotic kidneys. Diagnostic criteria used in categorizing the aetiologic factors were mainly clinical. They included the following: I. Hypertensive Nephrosclerosis (HTN) was diagnosed in those patients that were 40 years or older with history of HT in the previous 5 years, features of hypertensive heart disease (HHD), grade 3 or 4 hypertensive retinopathy, minimal proteinuria 1+ to 2+. II. Chronic Glomerulonephritis (CGN) was diagnosed in patients that were about 30 years (majority were younger than 25 years) with past history of acute or post infectious glomerulonephritis, nephrotic syndrome, recurrent body swelling, with moderate to massive proteinuria (>2+) . III. Diabetic nephropathy (DN) was diagnosed in those patients with diabetes mellitus (DM) diagnosed at least five years prior to presentation that also had proteinuria, hypertension, peripheral neuropathy, diabetic retinopathy and / or uraemic syndrome.
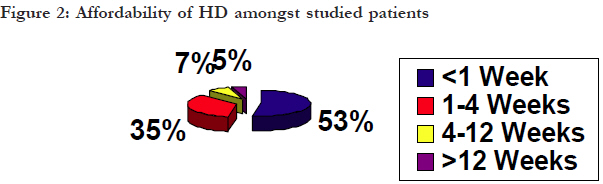
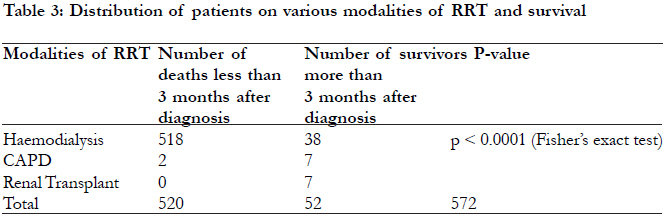
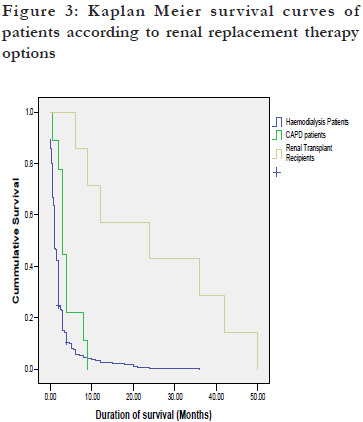
VI. Chronic tubulointerstitial nephritis (CTIN) was diagnosed in uraemic patients with significant analgesic consumption or exposure to metals, who had minimal oedema, and were either normotensive or had mild hypertension. VII. Patients that did not fit into any of these groups were classified as ESRD with undefined aetiology. Standard haemodialysis (HD) prescription included dialysis duration of 12 hours per week subdivided into three 4-Hour sessions or two 6-hour sessions depending on affordability. For continuous ambulatory peritoneal dialysis (CAPD), the typical prescription was 3-4 daily 2L exchanges and an overnight dwell. On the current costing of various RRT modalities, a session of HD costs about 130 USD while a day cycle of CAPD costs 80 USD. The cost of renal transplantation along with three months of immunosuppressive therapy is about 20,000USD. Statistical analysis Data was analyzed using SPSS package version 16. Measures of central tendency (mean, median) and measures of variability (range, standard deviation) were used to describe quantitative/continuous variables. Similarly, frequencies, percentages and cross tabulations were used to summarize qualitative variables. Chi Square and Fishers exact tests were used as appropriate to compare different groups. Kaplan Meier Survival curve was used to assess survival. Results A total of 13,668 medical cases were admitted during the period while 1,208 (8.83%) patients had ESRD. Of note was the fact that ESRD admissions constituted only 6.1% of medical admissions in 1989 and had increased to 21.5% in 2006 and 18.9% in 2007. Epidemiology and mode of presentation Of the 1,208 ESRD admissions managed over the period, only 760 (62.9%) case records were reviewed as the others were either not found or contained insufficient information. The age range was 15-90 years (median; 36 years), and there was a male preponderance with 534 (70.3%) being males. Ninety percent of the patients were from western Nigeria while 7% and 3% were from the east and north respectively. Major presenting features were body swelling in 67.8%, uraemic symptoms (nausea, vomiting, hiccups or pruritus) in 60.4%, and dyspnoea on exertion or orthopnoea in 33%. Although 40.7% of the patients had headaches only 20.8% of them had associated blurring of vision. Twenty-two percent had no past history suggestive of renal disease. A high proportion of patients (72.4%) had stage 2 hypertension (JNC VII) with median (range) systolic, diastolic and mean arterial blood pressures of 160 mmHg (120 – 270 mmHg), 100 mmHg (50 – 209 mmHg) and 120 mmHg (83.3–169.3 mmHg) respectively, only 34.1% had clinical cardiomegaly [Table - 1]. Seventy percent of those that had fundoscopic examination had either grade III or IV hypertensive retinopathy. Ascites and hepatomegaly were the commonest abdominal findings found in 55.3% and 39.2% respectively. Only 1.2 % of the patients had bone pains. Aetiology of ESRD Aetiology of ESRD found in the patients based on tubulointerstitial nephritis (2.2%), polycystic kidney our criteria outlined above included chronic disease (0.7%) and in the remaining 12% of the glomerulonephritis (43.7%), hypertension (31.1%), patients; the cause could not be ascertained [Table - 2]. One hundred and sixty one (21.2%) had exposure to nephrotoxic agents out of which 53.4% were herbal remedies. Of note is the progressive increase in the proportions of patients with CGN and diabetic nephropathy over the study period while the proportion of patients with HTN did not change over the period [Figure - 1]. Baseline serum chemistry in studied patients revealed median (range) serum creatinine, urea, potassium, sodium and bicarbonate of 1021 μmol/L (208 4728 μmol/L), 22.5 mmol/L (8.9 – 84 mmol/L) , 4.5 mmol/L (2.0 - 7.7mmol/L) , 132 mmol/L (104 -167mmol/L) and 19 mmol/L (12.0 - 30mmol/ L) respectively [Table - 1]. A high percentage of patients (50.8%) had serum creatinine above 1000 μmol/L at presentation while in 32.8% it varied between 500μmol/L and 1000 μmol/L and in the last 16.4% it was less than 500 μmol/L. Malnutrition was prevalent as 75.7% had hypoalbuminaemia (median for serum albumin; 31.0g/L (range: 10.9 – 46 g/ L)). Majority of the patients (88.9%) had anaemia with median packed cell volume (PCV) of 24.0% (range: 8.0-50 %). Twenty four percent of the patients had PCV of <20%, 64.9% had PCV between 20% and <33%, while in the remaining 11.1% it was greater than 33%. On serological screening, 95 (12.5%) of the patients were Hepatitis B surface Antigen (HBsAg) positive while only 15 (1.97%) and 12 (1.58%) were seropositive to Hepatitis C Virus (HCV) and Human Immunodeficiency Virus (HIV) respectively. During the period reviewed, these patients were managed conservatively as there was no dedicated machine for them. However, we now have dedicated machines for them but with strict barrier nursing. Management of ESRD and outcome Renal replacement therapy offered included haemodialysis (HD) in 556 (73.2%), CAPD in only nine(1.2%) patients and renal transplantation in only seven(0.9%). The remaining 188 (25%) patients were managed conservatively as they could not afford the various RRT options or were either HBsAg positive or seropositive to Hepatitis C Virus (HCV) or Human Immunodeficiency Virus (HIV) as our centre lacked dedicated machines for these categories of patients at that time. Payment for RRT in our setting is borne by patient’s out of pocket expenses, except major limiting factor for sustainability of RRT, out for the extremely few number of patients assisted of the patients managed with HD only 38 (5.0%) by corporate organisations or non governmental could sustain the treatment for more than 12 weeks. agencies. There is as yet no health insurance coverage These included 30 (3.9%) self sponsored patients for all modalities of RRT. Cost consideration was a and additional 8 (1.1%) patients supported by corporate or governmental agencies [Figure - 2]. Only these 38 patients survived on HD for longer than three months while seven CAPD patients and all transplanted patients survived for between six months and three years (P<0.00001) [Table - 3]. Majority (90%) of undialysed patients died within the first two weeks of presentation. Cause of death in most cases was advanced uraemia (70%) and congestive cardiac failure (25%) but was unexplained in 5% of cases especially those that discharged against medical advice and opted for care outside the hospital setting. Median duration of survival after diagnosis for all the patients was two weeks with range was 0 - 50 months. Kaplan Meier Survival Curve [Figure - 3] revealed that about 87% of our ESRD patients die in the first month of treatment and survival was significantly better in CAPD patients and transplant recipients. Discussion Chronic kidney disease (CKD) has assumed epidemic proportion worldwide hence its being regarded as a major public health challenge. While data on incidence and prevalence of CKD and ESRD are available in developed countries because of reliable and functional renal registries, they are either unavailable or unreliable in developing countries 1,2. Thus, the exact prevalence of CKD or ESRD in developing countries is unknown hence reliance on hospital derived data 8-12. In this study, which reviewed available data from 760 ESRD admissions (62.9%) of 1,208 ESRD patients seen over the 19 year period, ESRD admissions constituted 8.83% of total medical admissions. Of particular interest was the progressive increase in the percentage of ESRD admissions over the study period. Even though this is hospital data, it further support the increasing prevalence of CKD reported in community studies. In agreement with previous studies in SSA, our patients were young. This is in sharp contrast with reports from developed countries where CKD and ESRD affects the middle aged and elderly populations5,6,20,21. The male preponderance observed further supports findings from previous studies which may reflect the background prevalence of the predisposing illnesses and risk factors in males3,13,14. Socio-cultural and economic factors which preferentially favour males in our communities may also contribute. Even though the categorizations of the causes of CKD were mainly clinical without renal biopsies or autopsy reports, chronic glomerulonephritis and hypertension were the common aetiological factors in our setting. The occurrence of diabetic nephropathy is however increasing. This agrees with other reports from the sub-region and may reflect the high prevalence of chronic parasitic, bacterial, and viral infections particularly with the scourge of HIV / AIDS 4,7-17. In addition hypertensive nephrosclerosis remains a disease of blacks whose prevalence is not only high but is also increasing 9-14. Majority of ESRD patients in our setting, present late to the hospital. This was exemplified by the huge proportion of our reviewed cases that had features of uraemia even at first presentation. While this is similar to previous reports from SSA, it calls for urgent steps aimed at early detection and subsequent treatment10,12,17,22. Anaemia and malnutrition were also found to be common in our patients and may negatively impact on quality of life, cardiovascular disease and survival 23,24. The high prevalence of positivity to HBsAg reflect the high prevalence in the community and indicate that these categories of patients must also be offered different dialysis modalities. This has prompted the setting up of an isolation unit with dedicated machines for them but with strict barrier nursing. Despite the relatively low seropositivity to HCV and HIV observed, the patients should also be offered dialysis modalities and possibly transplantation if conditions are favourable. On the use of renal replacement therapies, majority of our ESRD patients had haemodialysis mainly because it was and still is the most readily available treatment modality 2. It is however sad to note that only 6.8% could afford the treatment for longer than three months principally because the cost (about 130 USD per session) is borne directly by the patients. As mentioned earlier, government subsidy is almost non-existent and the newly introduced National Health Insurance Scheme (NHIS) does not cover advanced care for renal disease including various modalities of RRT. This is a major reason for the very high mortality rate for ESRD in the subregion7,10,12,16. Only 1.2% had continuous ambulatory peritoneal dialysis (CAPD) (a day cycle of CAPD costs about 80 USD), and the major limitations to its continuous use included non-availability of consumables and very high infection rate 18,25. Similarly, renal transplantation whose cost along with three months of immunosuppressive therapy is about 20,000 USD, is still at its developmental stage in Nigeria as less than 1% of our patients could afford the procedure. In our series only 0.9% of our ESRD patients received renal allograft. The major limitations included funding, shortage of donor organs and lack of deceased organ donation as well as lack of appropriate legislation26. The prognosis for ESRD in SSA is still very poor as very few of our patients survived for longer than three months. Unfortunately, this is in agreement with previous studies 4,7,10,12,16,17,27. The risk of death is inexorably high in our subset of ESRD patients with a very high percentage dying within a few weeks of diagnosis. This situation is different in states with relatively freer and more equitable access to the various renal replacement therapy options either through health insurance or other state sponsored payment modalities 19,28-30. These high mortality figures should stimulate subsidy for and standardization of renal care in Nigeria and other developing countries. It should also herald commencement of preventive nephrology programs which could be primordial, primary, secondary or tertiary in all developing countries. The objectives of the prevention programs would be prevention or early detection of CKD, retardation of progression of CKD as well as appropriate planning for the initiation of various renal replacement therapy options 31. This would in the long term lead to a reduction in the number of patients that would require RRT, consequently leading to better survival and improved health related quality of life as well as a reduction in healthcare expenditure of the state. As much as possible, all prevention programs should include a treatment arm to be able to achieve these goals 31. Conclusion Advanced CKD presenting as ESRD is still prevalent with chronic glomerulonephritis and hypertension being the common causes and the prevalence of diabetic nephropathy is increasing. Presentation is late and prognosis and survival are still unacceptably poor. We therefore recommend that provision of renal replacement therapy in SSA should be supported and subsidized by governments, non-governmental agencies and health insurance companies where such exists. Renal transplantation should be encouraged in those that can support the treatment and above all preventive nephrology should be targeted in all underserved economies. References
Copyright © 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11117t1.jpg] [hs11117f3.jpg] [hs11117f2.jpg] [hs11117t2.jpg] [hs11117t3.jpg] [hs11117f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}