 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 12, No. 1, March, 2012, pp. 2-7 The evolution of haematological and biochemical indices in HIV patients during a six-month treatment period Mgogwe J1, *Semvua H3, Msangi R5, Mataro C2,4, Kajeguka D2,3, , Chilongola J2, 3
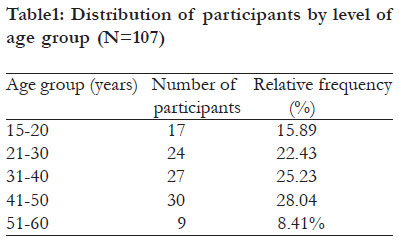
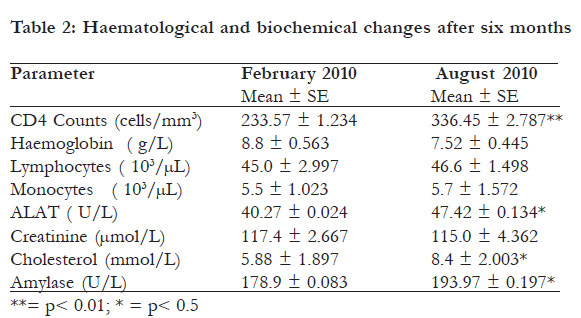
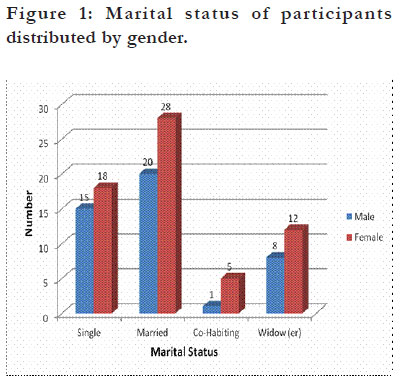
Code Number: hs12002 Abstract Objective: To assess haematological and biochemical parameters in Human Immunodeficiency Virus (HIV) patients under going antiretroviral therapy. Keywords: HIV; ARV; anemia Introduction HIV infection is associated with a wide range of haematological abnormalities. The peripheral blood findings and the morphological abnormalities in the bone marrow can simulate myelodysplastic syndrome, myeloproliferative disorders, and T cell lymphoma. Combination antiretroviral (ARV) therapy represents a major advance in the management of HIV type 1 (HIV-1) infection and is now a standard-of-care for HIV-1 infection. The disease is gradually fatal without ARV therapy but ARV therapy has effectively reduced morbidity and mortality of HIV-infected patients1. However the experience with ARVs is limited in Tanzania, as it is in most sub Saharan African countries. Infection with HIV-1 primarily involves a subgroup of T-lymphocytic cells, but other cell types are also invaded by the virus, including cell lines within the haematopoietic system. Together with infectious, inflammatory and neoplasic processes, invasion of haematopoietic tissue explains the haematological alterations which are seen during the course of infection with HIV-1. Anaemia develops in the larger proportion of patients. Thrombocytopenia frequently occurs during the course of the disease, but may be seen in some patients even at the time of diagnosis, where the condition may be misdiagnosed as “idiopathic” thrombocytopenic purpura. Neutropenia is seen in all disease stages, but is most severe in patients with advanced disease. Early reports have shown that patients treated very early on can recover or retain HIV specific CD4 + T cell response whilst maintaining an effective CD8+ T-cell response2 . In a related study conducted in 2005 in one hospital in Nigeria, it was observed that patients who started ARV therapy late, while their CD4+ cell count was <100 cells/mm3 didn’t respond well in ARV treatment compared those who started ARV therapy earlier and had extremely high biochemical parameters3 . A study was done in 2004 in Thailand on HIV/AIDS patients under ARV treatment at Chiang Hospital whose CD4+ count was <250 cells/mm3. After one month they were checked again, the haematological and biochemical parameters showed that about 70% of the patient under the study had returned to normal4 . It is known that ARVs, particularly those whose action inhibit viral proteases i.e. Protease Inhibitors (PI), are associated with adverse effects after long term use3. It was documented that all drugs used to treat HIV have side effects, for example some drugs change lipid level in blood thus causing high level of cholesterol. A previous study conducted in the UK on HIV/AIDS patient revealed that cytopenia is a common complication of infection with HIV type 1. Moreover, the study showed that in the cause of the disease more than 70% of the patients develop anaemia, sometimes requiring transfusion5 . Neutropenia, lymphopenia and thrombocytopenia are regularly seen. This indicates that more than one haematopoietic lineage may be impaired, with the degree of cytopenia being an indicator for severity of the disease in HIV/AIDS patients6 and bone marrow dysfunction being suggested as a likely mechanism. Adverse effects attributable to nevirapine have been reported as eosinophilia, granulopenia, jaundice, increase alanine transaminase (ALAT) and aspartate transaminase (ASAT), serum bilirubin and serum amylase. Anaemia, neutropenia and thrombocytopenia have also been reported as adverse effect of stavudine7 . With all the information above it shows the importance of evaluating the haematological and biochemical parameters in HIV/ AIDS patients under ARV therapy in order to monitor the body responses to the drugs. These responses may used as a monitoring tool for patients under ARV treatment. Therefore, assessment of haematological and biochemical changes in HIV/ AIDS patients under ARV therapy is of paramount importance. This study reports the first data that has evaluated selected biochemical and haematological adverse effects associated with the clinical use of ARVs in Tanzania. Methods The study enrolled both outpatient and inpatient HIV/ AIDS clients on ARV therapy at Bumbuli Lutheran Hospital in Tanga City, North Eastern Tanzania. To be enrolled in the study, participants were required to fulfill the following conditions: aged 18 years and above; must have laboratory evidence of HIV seropositive result, were eligible to start ARV, and absence of any serious chronic infection or disease. Participants were excluded if they were coming from outside the catchment area of Bumbuli Lutheran Hospital, were below 18 years of age, and patients ineligible for starting ARVs. Ethical clearance was obtained from KCMC research ethics committee (CRERC) and participants signed consent forms before samples were collected. The Bumbuli Hospital administration gave approval for the study to be conducted in the hospital. Patients under d4T or ZDV containing first line ARV drugs were followed for six months for changes in haematological and biochemical parameters from February to August 2009. Sampling was done at three points during the six month followup period at three month intervals. One milliliter of blood was collected and divided into two, 0.5 ml was put into a plain test tube and 0.5 into EDTA coated tube for biochemical and haematological assays respectively. Haematological analysis was done by using the 0.5 ml aliquot in EDTA coated tubes. Monocytes, lymphocytes, and Haemoglobin levels were determined using CelDyn 1600 Haematology Analyser (Abbott Diagnostics Inc., Il, USA). For biochemical analysis, whole blood stored in plain tubes was left to stand for one hour at room temperature (~25-30°C to allow it to clot. The sample was then stored at 4°C overnight to allow the clot to contact. Using a glass Pasteur, the clot was carefully loosened from the sides of the tube to avoid lysis of red blood cells. Centrifugation was done at 4000 rpm for 20 minutes at 4°C, then the clear serum was separated from the clot by pipetting off into clean labeled tubes using a glass pasteur. Serum was either analysed immediately or stored at -20°C. Commercial kits (DetectX®, Bio LAB,USA) were used to measure the activities of serum amylase and ALAT and to quantify serum creatinine and cholesterol. The procedure for, each test was followed according to manufacturer’s instructions. The ALAT catalyzes the transfer of amino group between L-Alanine and a Ketoglutarate to form pyruvate and glutamate. The Pyruvate formed reacts with NADH in the presence of Lactate Dehydrogenase to form NAD. The rate of oxidation of NADH to NAD is measured as a decrease in absorbance which is proportional to the ALAT activity in the sample. Absorbance was measured with spectrophotometer read at 490 nm and results calculated. Normal ranges were reported on the basis of the kits. The CD4+ cell count were determined for each patient at baseline, subsequently and during monitoring- using Facs machine adopted technique for CD4+ cell estimation under Nation ARV programme. The CD4+ cell count was expressed as cell/mm3 of blood. Data were generated for each patient at baseline and six months later. All data were collected and analysis was carried out using Statistical Package for Social Sciences (SPSS) version 16.0 (SPSS Inc., Chicago, USA). Continuous data were analyzed by the student t-test. Standard deviation (SD) and standard error (SE) were used to describe the spread around the mean. A p-value < 0.05 was considered the measure of statistical significance. Results A total of 107 participants were followed for six months of whom, 62 (57.94%) participants were females (table 1). Haematological parameters studied were CD4+ lymphocyte count, total lymphocyte count and haemoglobin levels during a period of six months after starting ARV therapy. Table 2 shows that, using students t test statistic, the mean CD4+ lymphocyte count increased significantly from 233.57± 1.234 in February to 336.45 ± 2.787(cells/ mm3) in August 2010 (p<0.01). A corresponding increase was observed with total lymphocyte count which increased from 45.0 ± 2.997 in February to 46.6 ± 1.498 (103 cells /μl) in August. However, this increase was not significant. We also observed an insignificant increase in monocyte count as presented in table 2 of results. The distribution of participants by level of their age groups indicates that most participants were between 31 and 40 years old, followed by the 41 to 50 category. The category between 51 and 60 years was least represented in the cohort. Severe anaemia (≤5g/dL) occurred in 24.7% of subjects while 75.3% were non-anaemic. Mean Hb in Feb was 8.8g/dL ± 0.563, while that of August, after six months of ARV treatment was 7.52 ± 0.445. This decrease was not statistically significant. Red cell morphology and pigmentation was seen to be variable with majority of the samples showing normochromic and normocytic (64%) while 36% showed hypochromia and anisopoikilocytosis. Leucopenia and thrombocytopenia occurred in 10/ 107 (9.3%) of the study population. The three biochemistry parameters studied (ALAT, amylase and cholesterol ) have shown significant increases during the six-month period of ARV use. The mean level of ALAT in February was 40.27 ± 0.024 U/L. In August ALAT was found at a mean leve of 47.42 ± 0.134 U/L. Similarly, amylase and cholesterol leves in February were 178.9 to 193 U/L and in 5.88 mmol/L, whereas these levels increased to 193.97 U/L and 8.4 mmol/L in August, respectively. Creatinine levels did not change significantly during the six month follow-up. Figure 1 shows that majority of participants (63/ 107 or 58.9%) followed in this study were females. 48 out of 107 participants (44.9%) were married. Discussion Antiretroviral therapy (ARV) has transformed the perception of HIV/AIDS from a plague to a manageable, chronic illness8-9. The ARVs have dramatically reduced the rates of mortality and morbidity as well as improved the quality of life for people living with HIV/AIDS. Despite ARVs being of extreme impact on the pathogenesis and health of most HIV/AIDS patients, issues of drug induced toxicities and their drug-induced haematological consequences (anaemia, neutropenia, and thrombocytopenia) and biochemical consequences have remained of great concern. Our study focused on evaluation of haematological and biochemical changes among HIV/AIDS patients under ARV therapy. Haematologic complications occur frequently in children with HIV infection and may be due to a variety of causes including HIV infection itself, and HIV-related conditions, or due to ARVs or other drugs. We show in our study a slight a decline of haemoglobin (hb) concentration in each individual over the follow-up period of six months. This implies that there was a tendency towards development of anaemia with continued ARV use. Previous studies show that haematological abnormalities are among the most common complications of infection with the HIV virus10. Adverse effects of ARVs are a major cause for non-adherence to medications. Anaemia is a well documented adverse reaction (ADR) in ARV use11. With the exception of haemolytic anaemia, the potential haematological toxicity of ARVs and combination treatments in HIV treated individuals has not been well established. Knowledge of the use and side effects of these drugs are crucial in the management of HIV-infected children as we scaleup the use of antiretroviral therapy9,11,12 Since ADRs such as anaemia have multiple etiologies, individuals with haematologic abnormalities should be evaluated for other pathophysiologic processes that might result in or contribute to anaemia, neutropenia, or thrombocytopenia. Conditions such as haemoglobinopathies or G6PD enzyme deficiency may contribute to haematologic adverse events. We show in our study that the overall mean CD4+ and total lymphocyte count increased with continued use of ARVs during the six months of follow-up, which is consistent with many previous findings13-17 . There is little consensus regarding the mechanism(s) by which CD4+ cell counts improve once ARV therapy is commenced. Antiretroviral therapy plays a critical role in halting the accelerated destruction of CD4+ cells which perhaps is the most widely accepted mechanism of HIV-associated CD4+ cell depletion. But there is also at least one other mechanism to ponder. This is impaired production of new CD4+ cells as a result of HIV infection-that may have significant bearing on the evaluation and potential use of various immunebased therapies during clinical management of HIVpositive patients. In this study, a significant increase in serum liver marker enzymes (ALAT, ASAT, and Alkaline phosphates) in HIV/AIDS patients was noticed. Liver transaminases are useful biomarkers of liver injury in individuals with some degree of intact liver function. Most liver diseases cause only mild symptoms initially, but it is vital that these diseases be detected early. Hepatic (liver) involvement in some diseases can be of crucial importance. The ALAT is found in serum and in various bodily tissues, but is most commonly associated with the liver. It catalyzes the transfer of an amino group from alanine to a-ketoglutarate, the products of this reversible transamination reaction being pyruvate and glutamate. It is commonly measured clinically as a part of a diagnostic liver function test. An increase in ALAT levels in serum may have crucial implications for individuals taking ARVs. It is of interest to note that HIV has been detected in the liver cells with, noticeable pathogenesis of the affected cells in infected individuals. Since HIV infection and AIDS patients tend to suffer more chronic forms of many secondary diseases and coinfections such as hepatitis B and C18 , it is therefore likely that the liver too will be affected and that subsequently, changes will occur in the activities of the liver enzymes in HIV infections and HIV AIDS patients. HIV attack host cells and take over control of the affected cells, leading to eventual death of the cells and subsequently the release of cellular contents into the surrounding medium. Although this may be regarded as an important explanation of ALAT elevations in HIV infected individuals19 , the possibility of ARV induced hepatotoxicity should not be overlooked. This is because if HIV was the only factor for elevated ALAT, it would be expected that with viral replication suppression by ARV drugs, serum levels of ALAT would go down. The observed increase may thus suggest the involvement of ARV-induced liver damage. A detailed analysis which could include differential enzymes studies, and a control HIV infected could clarify other sources of ALAT, ASAT and Alkaline phosphates increase in serum. Amylase and creatinine indicate degrees of pancreatic and renal damage respectively. There was an insignificant decrease in serum levels of creatinine during the follow-up period. However, we observed a steady increase in serum amylase levels during the six month follow-up period. The amount of creatinine excreted from the body is usually proportional to the total phosphocreatine content of the body, thus can be used to estimate muscle mass. When muscle mass decreases for any reason (HIV/AIDS, muscular dystrophy, paralysis, etc), both urinary and serum creatinine levels decrease. Our data indicate an insignificant creatinine deacrease to be a consequence of HIV infection associated muscle wastage, which is typical for HIV patients. The gradual elevation of amylase levels in serum indicate acute pancreatitis associated with ARV usage, in line with a previous study20 where nevirapine, one of the drugs used as first line drug in Tanzania and in this study, was attributed to pancreatitis. We report hypercholesteremia in patients under ARV treatment in six months of follow-up. While biochemical abnormalities may occur in individuals with body habitus changes, changes in lipid, carbohydrate and bone metabolism need to be given a separate consideration from those of change in physiognomy. This is because the pathogenesis of each may be different. Hyperlipidemia (elevated cholesterol and triglycerides) has been noted more commonly in individuals mainly under protease inhibitors (PIs) but also in many ARV types. Conclusion We conclude from our data that although the use of ARV increases the quantity of CD4+ cell counts, lymphocyte counts, and the lifespan of HIV patients, it however induces many un desirable ADR such as liver, kidney, pancreatic and lipocyte damage, and anaemia many of which could be due to a multitude of aetiologies. Recommendations This calls for a comprehensive assessment and management of HIV patients under ARV use. However, ARV increased the numbers of immune cells (CD4+ and total lymphocytes) significantly. The balance between the advantages and the side effects of ARVs should however not be something for debate, since nothing could be compared to debating on whether to live or not. Based on our findings, we recommended that haematological and biochemical data be collected regularly during the use of ARVs to enable personalised management of HIV infected patients. References
Copyright 2012 - African Health Sciences The following images related to this document are available:Photo images[hs12002t2.jpg] [hs12002f1.jpg] [hs12002t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}