 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 12, No. 1, March, 2012, pp. 17-25 Religiosity for HIV prevention in Uganda: a case study among Christian youth in Wakiso district *Kagimu M1,2,3, Guwatudde D 2, Rwabukwali C 4, Kaye S1, 5, Walakira Y1, Ainomugisha D1
Code Number: hs12004 Abstract Background: Utilization of religious institutions is one of the strategies for HIV prevention in Uganda. There is limited data on the association between religiosity and HIV infection rates.
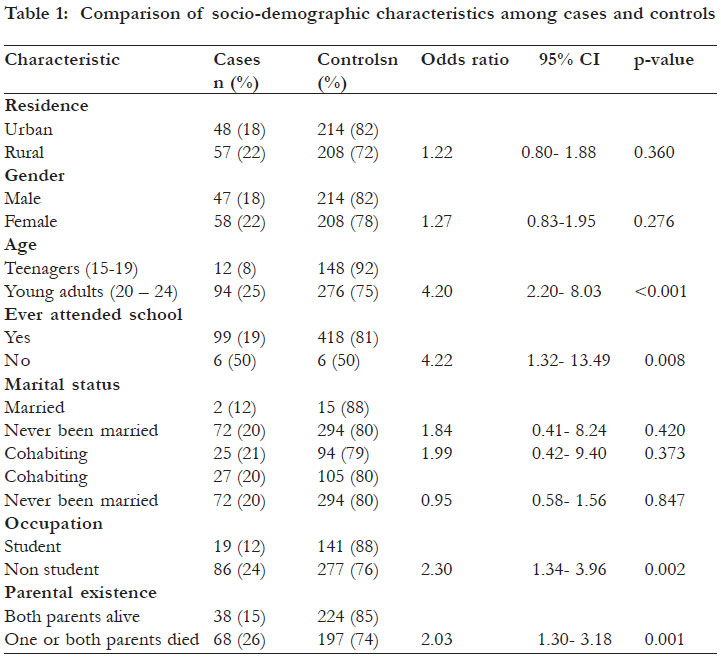
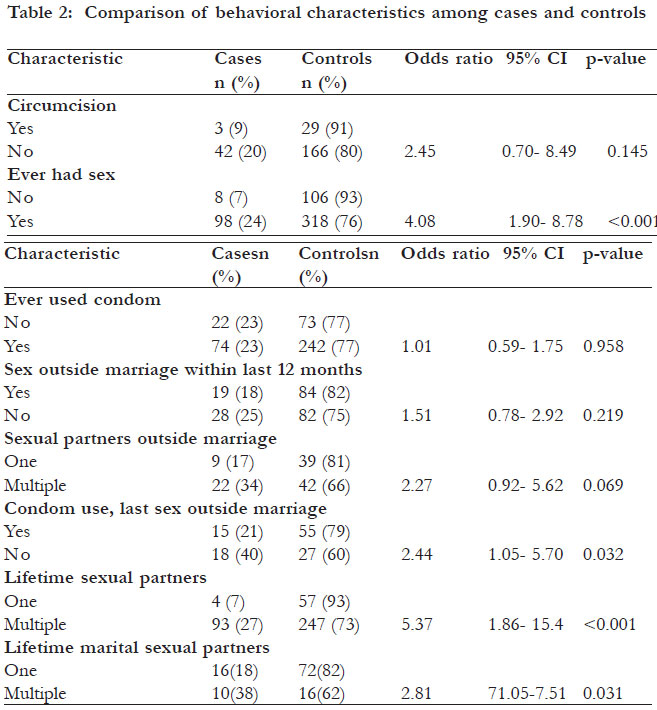
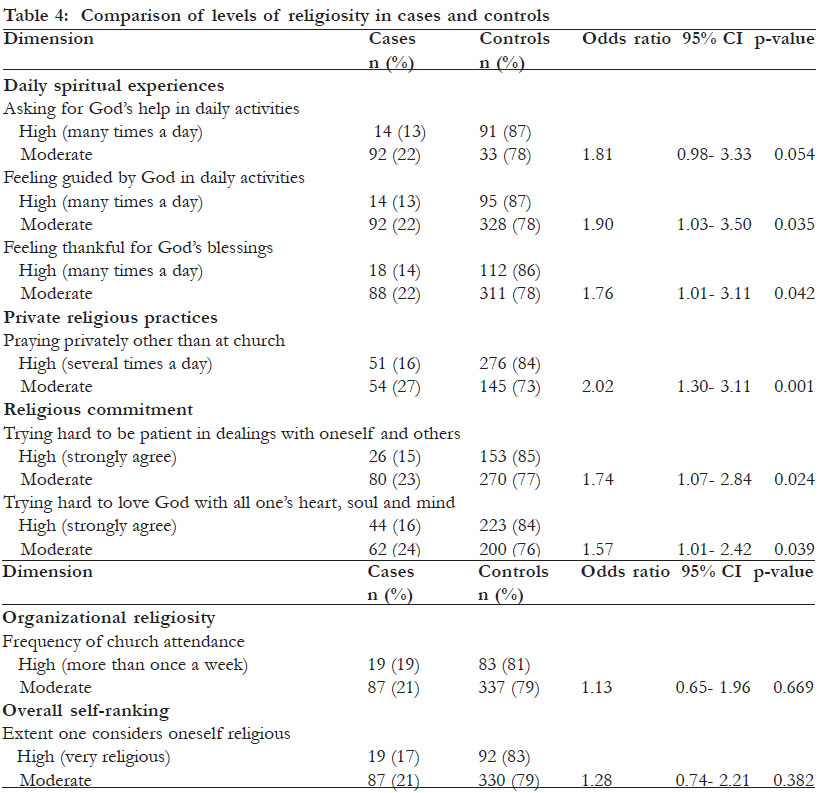
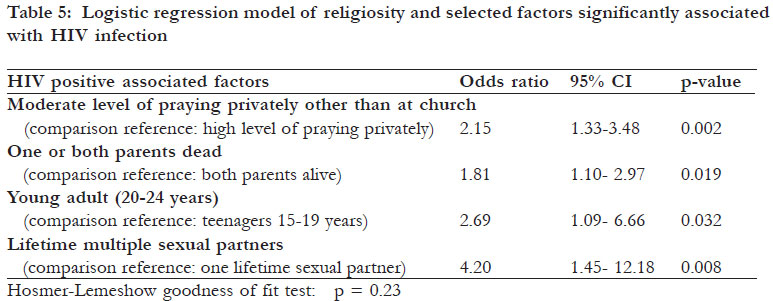
Key words: religiosity, HIV prevention, Uganda, Christians Introduction The HIV epidemic in Uganda is still a problem. The prevalence declined from a peak of 18% in 1992 to 6.1% in 2002. It has since stagnated for almost a decade between 6.1% and 6.5% in antenatal surveillance sites. Some HIV surveillance sites have shown an increase in HIV prevalence with deterioration in behavioral indicators such as an increase in multiple concurrent partnerships. The drivers of the epidemic include multiple sexual partners, inadequate condom use, inadequate circumcision rates, alcohol and drug abuse, and socio-cultural factors. The number of people estimated to be newly infected with HIV was 132 500 in 2005. In order to adequately address the problem of continuing new infections, it is recommended that evidence based planning and programming for HIV prevention interventions should be made. To achieve this, surveys with both serological and behavioral components should be conducted regularly to improve data availability 1,2. Utilization of religious institutions that are recognized promoters of religiosity in the community is one of the national strategies for HIV prevention 2. However, the empirical evidence for the role of religiosity in HIV prevention in Uganda is limited. Religiosity is defined by most scholars as an “individual’s or group’s intensity of commitment to a religious belief system” 3. It is thought that faithbased organizations can play a significant role in promoting behaviors supportive of HIV prevention, such as abstinence from sex before marriage and being faithful in marriage for accordance with religious teachings 4. Indeed it is conceivable that in Uganda, these organizations such as Islamic Medical Association of Uganda for the Islamic faith, Church Human Services for the Anglican faith, the Catholic Church and other churches could have played a significant role in promoting behaviors that led to the decline of HIV infections in the 1990’s. There is limited data regarding this issue. One study reported that high religiosity was associated with a low level of premarital sexual permissiveness among Ugandan communities 5. In another study, when mosque leaders (Imams) were supported to deliver an HIV/ AIDS health education intervention, there was a significant reduction in self reported sexual partners among respondents aged less than 45 years after two years of implementation 6. There is also limited data regarding the possible relationship between religiosity and the prevalence of HIV infection. In the Uganda national serobehavioral survey of 2005 only elementary questions about religious denominations were asked. It was found that the prevalence of HIV infection differed among denominations being 7.1% among Protestants, 6.3% among Catholics and 5.0% among Muslims 7. It is possible that religious practices such as circumcision could partly explain the differences. However, it is not clear whether those who are more religious and adhere to their religious practices have a lower HIV prevalence rate compared to those who do not. It has been suggested by scholars that studies linking religiosity to serological markers of HIV infection are likely to increase understanding of the role of religion in HIV prevention 8. Such studies have not been undertaken to a large extent in Uganda to a large extent. The objectives of the study were to determine factors likely to be driving the epidemic and assess the association between religiosity and HIV prevalence rates among Christian communities. Methods Study setting and sampling The Islamic Medical Association of Uganda (IMAU) which is a faith-based non-governmental organization has been running a hospital called Saidina Abubakar Islamic Hospital located at Wattuba in Wakiso district, 14km from Kampala city on Bombo road, since 2005. In addition, IMAU staff have been working with both Muslim and Christian religious leaders to educate communities around the hospital on issues of HIV prevention and control. The education curriculum includes scientific knowledge supported by faith teachings 9. IMAU staff also perform home-based HIV counseling and testing for communities surrounding Saidina Abubakar Islamic Hospital. Communities from 30 mosques and 30 churches around the hospital were identified to participate in the study. A convenience sample was therefore used for the study. Study design The study design was an unmatched case-control study, to assess the association between religiosity and HIV infection rates. In this study design it is new (incident) cases that are preferred for the analysis, although prevalence rates have been used by some scholars 10. The prevalence of HIV in young people who are 15-24 years old is a reasonable proxy indicator of incident cases 11. The prevalence of HIV infection in this age group in Uganda is low at 3.4% according to the 2005 sero-behavioral survey 7. A case-control study is therefore best suited for studying such rare cases of HIV infection in this age group 12. The sample size was calculated using a formula for unmatched case-control studies with multiple controls per case 13. It was estimated that the proportion with higher religiosity among the controls would be 50% with a relative risk of 0.5. As a result of a low prevalence of HIV infection in the targeted age group, it was anticipated that many people would have to be screened before cases were identified. In view of the limited resources it was decided to use four controls per case, in order to reduce the number of cases required while increasing the power of the study. It has been calculated that beyond four controls per case there is limited additional power gained in a study 14, 15. The sample size was calculated to be 100 cases and 400 controls. Because of different religious traditions it was planned that Muslims and Christians be analyzed separately but with the sample size calculated in a similar way for each group. Selecting cases and controls Cases were defined as clients between 15-24 years who were HIV positive. They were identified by performing home-based HIV counseling and testing in homes surrounding a place of worship that had clients in the selected age group. On average between 50 - 100 clients were tested in homes surrounding each place of worship. Controls were defined as clients who were HIV negative. They were selected at the end of the study as a random sample from HIV negative Christian respondents who had been tested. Measurements HIV testing was done by IMAU nurses and counsellors as well as laboratory staff from Saidina Abubakar Islamic Hospital. Rapid test kits were used in accordance with the Uganda Ministry of Health guidelines16. The blood was first tested using Determine HIV- 1/2 (Abbot, Tokyo, Japan) rapid test kit. For an HIV negative test result no further test was done. For an HIV positive result another test was done using the HIV-1/2 STAT-PAK (Chembio, Medford, NY) test kit. If this test was positive, the client was recorded as HIV positive. If the result was negative a third test was done as a tie breaker using Uni-Gold Recombigen HIV test (Trinity Biotech, Wicklow, Ireland). If this gave a positive result the client was recorded as HIV positive and if it was negative the client was recorded as HIV negative. Religiosity Religiosity was measured using a modified Brief Multidimensional Measure of Religiousness/ Spirituality. This instrument is published by John Fetzer Institute in Michigan USA in a document entitled: Multidimensional measurement of Religiousness/Spirituality for use in health research The publishers indicate that it may be used and reprinted without special permission. The authors recommend a flexible approach for using the instrument which includes measuring selected domains or using selected items to measure a dimension of interest17. This instrument was found to have good validity and reliability among adolescents in Boston, USA18. from the instrument, questions were selected on daily spiritual experiences, private religious practices, organizational religiosity, overall self-ranking of religiosity, religiosity history, and religious commitment. Other questions were added to measure more aspects of religiosity that were thought to be relevant to the target communities. The measures of religiosity were ordinal variables so that the degree or intensity of religiosity could be determined from the responses. The questionnaire was translated into Luganda, the local language of the target communities and the IMAU hospital staff who were trained in how to administer it to respondents. The questionnaire was tested on three hundred respondents and the measures of religiosity were found to have adequate validity and reliability. Socio-demographic factors and HIV-risk behaviors and practices The questionnaire had items for data collection on socio-demographic factorss as well as behaviors and practices related to HIV infection. Statistical analysis Double data entry was done in EpiData statistical package version 2.1b. The data were cleaned and the final data set made. Statistical analysis was done in STATA 10 computer program. The information was organized into categorical frequency data and the Chi square test used to test significance between groups. A p-value less than 0.05 was considered significant. Ethical considerations The study was approved by Makerere University School of Public Health Institutional Review Board, as well as Uganda National Council of Science and Technology. Results HIV infection rates and socio-demographic characteristics From July to December 2010 a total of 4 268 clients between 15 and 24 years were interviewed and tested for HIV infection, of whom 2 933 were Christians. There were 106 cases with HIV infection giving a prevalence rate of 3.6%. A random sample of 424 clients was selected as controls from among the HIV negative respondents. The socio-demographic characteristics of the cases and controls are shown in table 1. HIV infections were significantly associated with being a young adult of 20-24 years (odds ratio 4.20, 95%CI 2.20-8.03, p<0.001); not having attended school at all (odds ratio 4.22, 95%CI 1.32-13.49, p=0.008), being out of school as a nonstudent (odds ratio 2.30, 95%CI 1.34-3.96, p=0.002); and having lost one or both parents (odds ratio 2.03, 95%CI 1.30-3.18, p=0.001). Behavioral characteristics and HIV infection rates The association between HIV infections and selected sex-related behavioral characteristics is shown in tables 2 and 3. HIV infections were significantly associated with those who had ever had sex (odds ratio 4.08, 95%CI 1.90-8.78, p<0.001); those who had multiple life-time sexual partners (odds ratio 5.37, 95%CI 1.86-15.47, p<0.001); those who had multiple lifetime marital sexual partners (odds ratio 2.81, 95%CI 1.05-7.51, p=0.031); and those who did not use condoms in last sex outside marriage within the last 12 months (odds ratio 2.44, 95%CI 1.05-5.70, p=0.032). Other behaviors associated with higher HIV infection rates included those who had ever had sex during menstruation (odds ratio 1.83, 95%CI 1.07-3.15, p=0.025); those who had ever drank alcohol (odds ratio 2.28, 95%CI 1.433.65, p<0.001); those who ever drank alcohol before sex (odds ratio 2.83, 95%CI 1.57-5.11 p<0.001); and those who ever used narcotic drugs for recreation (odds ratio 2.49, 95% CI 1.14- 5.44, p=0.018). Religiosity was measured using ordinal variables. For himself or herself. The statement used for this example, regarding the dimension of daily spiritual measurement was “I feel guided by God in the midst experiences related to feeling guided by God in daily of daily activities”. The levels of religiosity to select from in descending order of intensity were: 1. many times a day, 2. every day, 3. most days, 4. some days, 5. once in a while, 6. never or almost never. Among the controls, the responses to this question were as follows: 1. many times a day 95(22%), 2. everyday 262(62%), 3. most days 40(9%), 4. some days 17(4%), 5. once in a while 7(2%), 6. never or almost never 2(1%). This was a typical response among cases and controls on measures of religiosity, indicating that the majority of respondents were quite religious people. For the purpose of comparison, the respondents were divided into two groups; group 1 was those with high religiosity who gave the highest level category 1 response and group 2 was those with moderate religiosity, who gave the remaining responses of categories 2-6. Since there were very few respondents with the lowest levels of religiosity, they were included in group 2 for the sake of data analysis The association between religiosity and HIV infections is shown in table 4. There were several dimensions of religiosity, where those with lower levels of religiosity had significantly higher HIV infection rates. Those who did not feel guided by God in the midst of daily activities many times a day had higher HIV infection rates, compared to those who did (odds ratio 1.90, 95%CI 1.03-3.50, p=0.035). Those who did not feel thankful to God for their blessings many times a day had significantly higher HIV infection rates compared to those who did (odds ratio 1.76, 95%CI 1.01-3.11, p=0.042). Respondents who did not pray privately in places other than at a church several times a day had significantly higher HIV infection rates compared to those who did (odds ratio 2.02, 95%CI 1.30-3.11, p=0.001). Over 90% of those who prayed privately other than at a church several times a day reported praying between two to four times per day. Respondents who did not strongly agree that they tried hard to be patient in dealing with themselves and others in accordance with their religious teachings, had significantly higher HIV infection rates compared to those who did (odds ratio 1.74, 95%CI 1.072.84, p=0.024). Those who did not strongly agree that they tried hard to love their God with all their heart, soul and mind in accordance with their religious teachings also had significantly higher HIV infection rates, compared to those who strongly agreed with this proposition (odds ratio 1.57, 95%CI 1.01- 2.42, p=0.039). Association between HIV infection and combined factors A logistic regression model which shows significant associations between HIV infection and selected statistically significant factors found in bivariate analysis is shown in table 5. Higher rates of HIV infections were concurrently significantly associated with a moderate level of praying privately (odds ratio 2.15), loss of one or both parents (odds ratio 1.81), being a young adult (odds ratio 2.69), and having multiple lifetime sexual partners (odds ratio 4.20). This suggests that some religious dimensions such as praying privately at places other than a church may independently influence HIV risk behaviors, which then determine HIV infection rates. Discussion The HIV prevalence among Christian youth aged between 15 and 24 years old who were studied was 3.6%. This rate is similar to the prevalence of 3.4% that was found earlier in 2005 during the national sero-behavioral survey 7. The socio-demographic drivers of the epidemic in this community include being a young adult, never having attended school, being out of school, and having lost one or both parents. The behavioral factors driving the epidemic include having sex, multiple sexual partners, not using condoms in sex outside marriage, sex during menstruation, drinking alcohol, and using narcotic drugs for recreation. These drivers are similar to what has been documented 1. When some dimensions of religiosity were reported to be at lower levels by respondents, they were significantly associated with higher HIV infection rates in these communities. These dimensions include feeling guided by God in daily activities, feeling thankful for God’s blessings, praying privately several times a day in places other than at a church, trying hard to be patient in dealing with oneself and others, and trying hard to love God with all one’s heart, mind, and soul. These findings are consistent with the expected higher sexually transmitted infection rates including HIV infections, among people who are less committed to their religious teachings 19. On the whole, the risk of having HIV among respondents with lower levels of these religiosity dimensions was about twice that of respondents with the highest levels. The most significant measure of religiosity associated with higher HIV infection rates was a lower level of private prayer. When it was combined in a logistic regression model with some drivers of the epidemic including multiple sexual partners, loss of one or both parents and being a young adult, it still remained a significant factor. This suggests that this religiosity dimension may independently influence HIV risk behavior, which then determines HIV infection rates. These empirical data support inclusion of the issue of religiosity in HIV prevention strategies. People who have higher levels of some dimensions of religiosity and are committed to their religious belief system have a lower risk of getting HIV infection. The mechanism for this is thought to be through self-control. Religion is a primary regulator of human behavior, capable of controlling impulses towards short term individual gain in the interest of the long term good 20. Religion sets definite standards of right and wrong as a way for people to identify acceptable guidelines for behaviors. Religion also provides the motivation for adhering to the standards. Calling people to pursue a deeper meaning to life rather than the satisfaction of selfish desires, followers are inspired to identify with the values and priorities of a given religious tradition 21 The data in the study also support the strategy of the faith- based approach to HIV prevention, which involves education of communities using scientific knowledge supported by religious teachings 9. As an example of this, praying privately several times a day was significantly associated with lower HIV infection rates. Religious teachings from the Holy Bible, relevant to this dimension, can be used to increase this behavior in the target communities. An example of this from the Holy Bible is the teaching of Jesus Christ as follows: Holy Bible: Matthew 6: 5-13.
The study has provided empirical data on one of the values of this faith teaching. The Christians who were less committed in following this teaching had significantly higher HIV infection rates. Religious leaders who are an essential component of the faithbased approach to HIV/AIDS may use this data to reinforce their messages for HIV prevention for their communities. This study had limitations in detecting differences between different levels of religiosity. Additionaly, the study instrument was administered to respondents by interviewers. Most Ugandans are religious people in accordance with Uganda’s motto which is “For God and my country” and is enshrined in the Constitution 22. Appearing to be religious is therefore socially desirable in Uganda. This means that some respondents could have given socially desirable answers to the questions which may not reflect the true level of their religiosity 23. On the other hand, many respondents could have been quite religious, making it difficult to detect the small differences in religiosity between individuals. The association of some dimensions of religiosity with HIV infection may therefore not have been detected for this reason. Conclusion Lower levels of several dimensions of religiosity are significantly associated with higher HIV infection rates. This provides empirical data for strengthening religiosity in HIV prevention strategies among Ugandan Christian communities. Acknowledgements We are grateful to the communities in Wakiso district who participated in this study. We would also like to thank all the staff of Saidina Abubakar Islamic Hospital who participated in data collection, entry, and analysis for the study. The support given to us by Makerere University School of Public Health-CDC/HIV/AIDS Fellowship program is very much appreciated. References
Copyright 2012 - African Health Sciences The following images related to this document are available:Photo images[hs12004t4.jpg] [hs12004t3.jpg] [hs12004t2.jpg] [hs12004t5.jpg] [hs12004t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}