 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
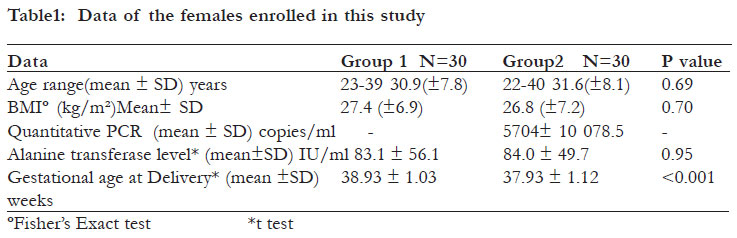
African Health Sciences, Vol. 12, No. 1, March, 2012, pp. 58-62 Hepatitis C virus (HCV) status in newborns born to HCV positive women performing intracytoplasmic sperm injection *Nesrine F, Saleh H Faculty of Medicine - Medical Microbiology and Immunology, Khartoum square Azarita Alexandria, Egypt Code Number: hs12010 Abstract Background: A low risk of HCV vertical transmission has been reported especially in those born to women with viraemia. Intracytoplasmic sperm injection (ICSI) being an assisted reproduction technique includes procedures that may increase risk of transmission. Key words: intracytoplasmic sperm injection, hepatitis C virus Introduction Hepatitis C virus (HCV) infection is a parentrally transmitted viral infection affecting liver with a 3% universal prevalence, with predominance within the Middle East1. The described natural history of the virus is characterized by a high rate of chronicity of up to 70%, with a high association with development of hepatocellular carcinoma2. A low risk of HCV vertical transmission to the newborns has been reported specially in those born to women with high levels of viremia3. Infertile HCV carrier females are usually accepted in the assisted reproduction techniques (ART) programms of many fertility centers. Studies have demonstrated HCV RNA in follicular fluid of HCV polymerase chain reaction (PCR) positive females4. Furthermore, HCV RNA can be detected in semen of males with high blood viral load. However, still no evidence for sexual transmission was reported5. Studies have demonstrated that purification of semen by density gradient eliminates chances for viral RNA detection on sperms6. All around the world, HCV positive males and/or females have been accepted in many fertility centers for assisted reproduction. Intracytoplasmic sperm injection is usually performed in such cases, with precaution taken to avoid HCV transmission inside the lab5-9. To diagnose HCV infection in infants, molecular methods as detection of viral RNA using PCR is the test of choice as maternal antibody to HCV can be detected in the serum of babies born to anti-HCV antibodies (Ab) positive mothers, up to 13 months after delivery. ObjectiveTo determine the rate of vertical transmission of hepatitis C virus to newborns born to HCV positive mothers in ICSI cycles. Methods A cross-sectional observational study was done. As a routine practice in our fertility center, couples are tested for HCV antibody and for HCV RNA in serum via real time RT-PCR. Serum samples were collected within the first week after labor, from newborns of two groups of ICSI cycles pregnant females in the period from July 2004 and July 2009: Group one included 30 females with sera anti-HCV antibody positive and PCR negative. .All male partners of the females included in this group have been found both anti HCV antibody and HCV RNA negative. Group two included 30 female anti-HCV antibody positive with PCR positive (i.e.: virus present in blood). Only two male partners, of females belonging to group 2, were positive for anti-HCV antibody and negative for PCR for HCV RNA. Neither frozen oocytes nor frozen embryos originating newborns were included in this study. Only live births were included in our study. Couples whose newborns were selected to be enrolled in our study have been informed and consented prior to delivery according to the local regional ethical committee advice. Newborn sera were subjected to anti-HCV antibody testing via a chemiluminescence antibody testing assay (Cobas,Roche)10, and to testing of presence of HCV viral RNA via a Real time RT-PCR. Extraction of the samples for the RT-PCR was performed using QIAamp RNA minikit (Qiagen). Real time quantitative PCR was performed in Stratagene thermal cycler using specific Primers and Taqman probe ( Qiagen) for HCV amplification11 . All the precautions were taken in the embryology laboratory to avoid HCV transmission between the gametes inside the laboratory, including separate consumables to each case7-9 eg. injecting and holding pipettes, flexipettes, etc. All semen samples for ICSI were routinely prepared via sperm gradient method. A minimum number of one and a maximum of three best embryos were selected for transfer after 48 hours post ICSI. Embryo transfer was performed under ultrasound guidance using a Labotect embryo transfer catheter. Statistical analysis Statistical analysis was performed using Statistical Package for Social Sciences (SPSS/version 15) software. The statistical tests used were as follows: arithmetic mean and standard deviation; for categorized parameters, the Fisher’s exact test was used, while for numerical data the t-test was used. The level of significance was 0.05. Results It was found that the quantitative RT –PCR of the females belonging to group two ranged from 200 to 16 000 copies/ml with the mean and standard deviation of 5 704 and 10 078.5 respectively. All newborns included in this study were delivered via an elective cesarean section for purpose of decreasing the risks of hepatitis C virus vertical transmission after counseling and consenting of the parents. Out of all ICSI cycles ending in live births within the study period, deliveries of HCV positive females constituted less than 0.5% of all deliveries. Data concerning the females enrolled in the two studied groups is summarized in table 1, with no significant difference between the two groups regarding age, body mass index (BMI), and alanine transferase serum level. In group one female newborns born from 30 deliveries were 33, as three cases had twins. In group two, the newborns were 33 as one female delivered triplets and one had a twin. Out of the newborns to 30 females; anti-HCV antibody positive and PCR negative none was positive for anti-HCV antibody, nor for Reverse transcriptase-PCR for Hepatitis C virus RNA. Only one newborn (that resulted from a singleton pregnancy) was born to one female belonging to group one positive for anti-HCV Antibody and PCR positive for HCV. Discussion Studying the possible transmission of different infectious agents via assisted reproduction procedures has been a concern to many researchers.9 Guidelines for a good ART practice emphasize for screening for both partners for a list of infectious agents that carry the possibility of being transmitted through gamete manipulations and transfer12. Hepatitis C virus is one of the parentrally transmitted infectious agents that is characterized by a high rate of chronicity.13 Some HCV seropositive patients can conceive naturally while others are infertile and may seek for assisted reproduction. Studies demonstrated that it does not affect the pregnancy13, while others reported that hepatitis C positivity may affect success of assisted reproduction 14. There are rising concerns to demonstrate the possibilities for HCV transmission from mother to child in such conditions. The reported rates of vertical transmission to the newborns from HCV positive mothers are characterized by discrepancies between recent earlier ones 9,14. Many researchers investigated the incidence of HCV transmission in between gametes by detection of viral RNA in many settings of the procedure15-17 . However, no studies have been carried out to record the transmission rate to the newborns after micromanipulation techniques to the gametes. As many authors reported the detection of the HCV RNA in the follicular fluid, we speculated that HCV could have higher vertical transmission from HCV positive females undergoing ICSI18. Michielsen et al, 19993 reported a very low (1%) vertical transmission of HCV from females that are HCV RNA negative in natural conception, while in cases with HCV RNA positivity the transmission rate increased to 11%. In agreement, Van der Poel et al19 also noted the low mother-tochild transmission in chronic carriers and which occurs mostly during the initial viremia during pregnancy. Other researchers reported that the risk of vertical transmission of HCV appeared to be related to the level of viremia in the pregnant mother. The virus does not appear to be transmitted when a woman’s titer is less than 106 copies/ml20-22. Although some researchers did not find that the route of delivery affects the rate of HCV vertical transmission23,24, still other researchers reported a lower HCV maternal to child transmission rate in case of delivery by elective cesarean25. In our study, the vertical transmission of HCV virus in case of conception from ICSI cycle did not seem to be higher than the reported rates of transmission in case of natural conception. The ICSI procedures in this study have been following the precautions to guard against HCV transmission in between gametes provided in the guidelines for good practice of ART of the European society of human reproduction and embryology9. In our study only one newborn was found to be PCR positive to HCV during the first week after delivery. We did not include a longer follow up of the cases (due to lack of access to the parents). In the view of the natural history of HCV , approximately 75% of acute cases become chronic 26 while 25% of cases appear to clear HCV infection. Nevertheless, they have persistent HCV antibodies, though in the latter no detectable viremia, and studies show that small amounts of the virus may still be detectable in leukocytes and hepatocytes 26,27 . Conclusion Hepatitis C virus vertical transmission in pregnancies from ICSI cycles seemed to be of very low incidence in PCR positive females, while the transmission of HCV to the newborns from HCV PCR negative sero-positive females appeared to be completely absent. This observation could have an impact on the clinicians’ counseling for HCV positive females seeking ICSI. African Health Sciences Vol 12 No 1 March 2012 References
Copyright 2012 - African Health Sciences The following images related to this document are available:Photo images[hs12010t1.jpg] |
| |||||||||

{kind=link}