 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 12, No. 1, March, 2012, pp. 81-86 Cross-sectional pilot study about the health status of diabetic patients in city of Misurata, Libya * Elhwuegi AS1, Darez AA2, Langa AM2, Bashaga NA2
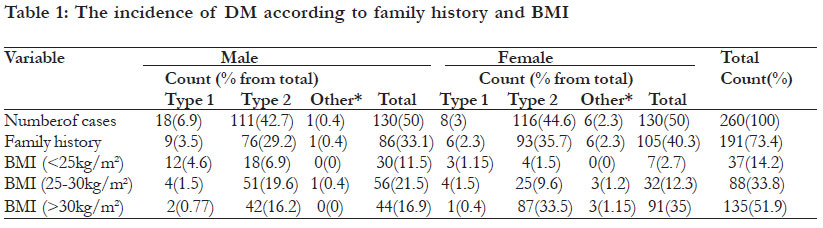
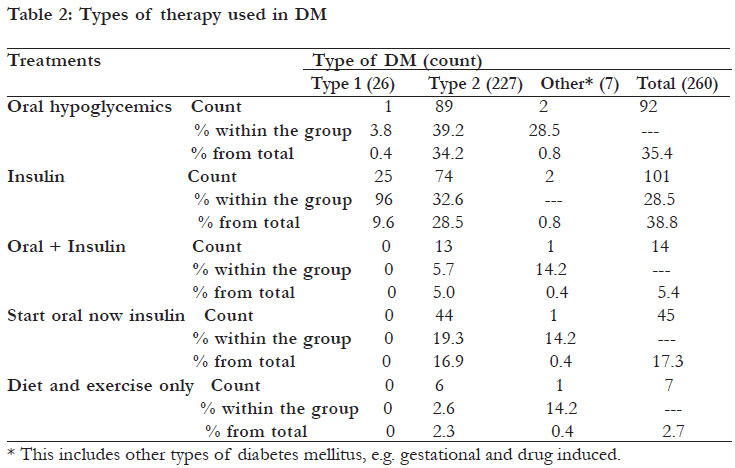
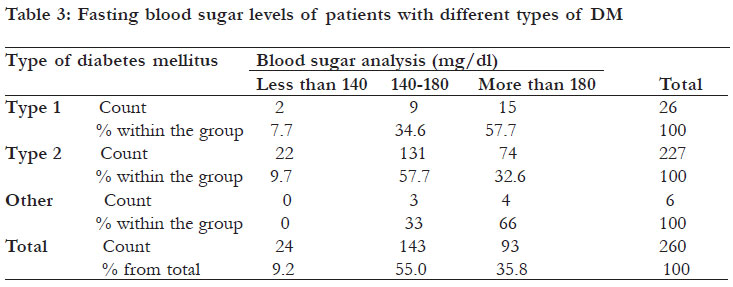
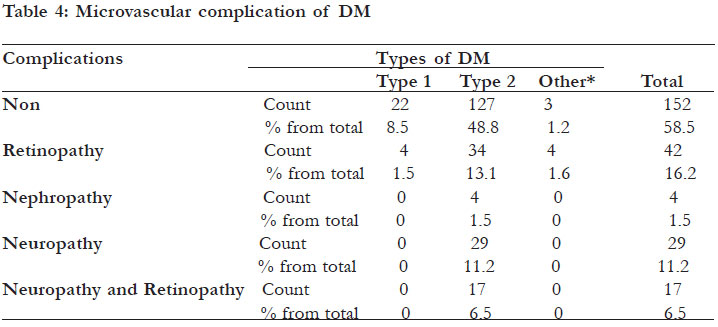
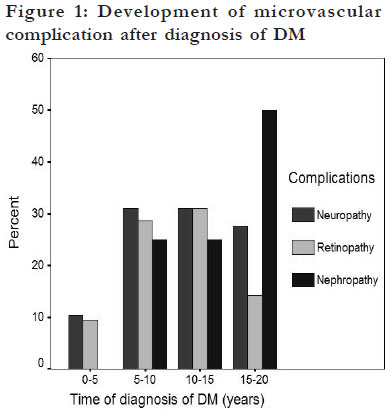
Code Number: hs12015 Abstract Background: Being a leading cause of death worldwide, epidemiological studies about diabetes mellitus have encouraged governments to initiate or improve local diabetes monitoring and prevention strategies. Key words: diabetes mellitus status, Misurata, Libya Introduction Diabetes mellitus (DM) is characterized by chronic hyperglycemia with disturbances in carbohydrate, lipid and protein metabolism. The world wide prevalence of DM for all age groups is set to increase from 2.8% in 2000 to 4.4% in 20301. Uncontrolled DM may result in several dangerous complications involving most body organs including retinopathy, nephropathy, neuropathy and cardiovascular diseases2. Diabetes is now among the leading causes of death due to diseases in most countries of the world3. Therefore DM is a growing public health problem all over the world. Epidemiological studies about DM have encouraged governments to initiate or improve local diabetes monitoring and prevention strategies. Misurata is fast growing city in the north of Libya with a district population of just over 550,000 in 2006 and it is considered to be the third largest city in Libya after Tripoli and Benghazi. No research could be found about the profile of diabetes mellitus in this city. It was decided therefore to carry out a pilot study involving diabetic patients visiting a specialized centre in Misurata in order to study the general profile of the disease including risk factors and complications. Methods This study is a cross-sectional observational pilot study about the profile of diabetic patients visiting the specialized centre for management and treatment of diabetes and endocrine disorders, Misurata -Libya. The numbers of diabetic cases studied were 260 cases (130 females and 130 males) randomly selected from the total number of patients visiting the centre for the period between January 2008 and March 2008. Data were collected from patient files and by directly questioning the patients. The information included a detailed history about the patient (including body mass index BMI), type of DM, types of treatments used, time of diagnosis of DM, fasting blood sugar, education levels, complications of DM and time of their appearance after diagnosis. The data collected was presented on a spreadsheet using SPSS software program version 13. The frequency (count) for the specific variable and its percentage of occurrence within all patients and/or within the group (type 1 or type 2 DM) were calculated. The same software was used for the tabular and graphical presentations of the data. Results Types of DM and family history The majority of the diabetic cases (87.3%) belonged to type 2 DM with nearly equal percentage in male and female patients (42.7% and 44.6% respectively). 9.9% of the patients had type 1 DM with higher percentages in males (6.9%) than in females (3%). 73.4% of all patients had a family history of diabetes (40.3% in females and 33.1% in males) (Table 1). Association of DM with body mass index (BMI) It was found that 51.9% of all diabetic patients were obese (BMI > 30 kg/m2), 33.8 % were overweight (BMI 25-30 kg/m2) and only 14.2% were lean (BMI < 25 kg/m2) (Table 1). When a comparison was made between the type of DM and BMI, it was found that 57.7% of Type 1 diabetic cases (15 out of 26) were lean, 30.7% (8 out of 26) were overweight, while only 11.5% (3 out of 26) were obese. On the other hand, 56.8% of type 2 diabetic cases were obese (129 out of 227), 33.5% were overweight (76 out of 227), while only 9.7% were lean (22 out of 227). The percentage of female obese type 2 patients was much higher than the percentage of male obese type 2 patients (33.5% versus 16.2% respectively). On the contrary, the percentage of overweight male patients was higher than percentage of overweight female patients (19.6% versus 9.6% respectively). Age groups of diabetic patients It was found that 85.7% of all diabetic patients (223 out of 260) were above 40 years old with the highest frequency seen in the age group 50-70 years old. Almost all patients with type 2 DM were above 30 years old (218 out of 227), while most of Type 1 DM were below 30 years old (19 out of 26). Types of treatments of DM As a whole, 38.8% of all diabetic patients were treated with insulin, while 35.4% of the patients were treated with oral hypoglycemics. On the other hand, it was found that 17.3% of the patients were started on hypoglycemics and then changed to insulin. 2.7% of the patients were on diet and exercise alone, while 0.4% were started with insulin then changed to oral hypoglycemics (table 2). Only 39.2% of the patients with type 2 DM (89 out of 227) were treated with oral hypoglycemics while 32.6% of these patients (74 out of 227) were treated with insulin and 5.7% (13 out of 227) were treated by both classes. On the other hand, 96.2% of type 1 diabetics (25 out of 26) were treated with insulin and only one diabetic patient (3.84% of type 1) was treated with oral hypoglycemics (table 2). Fasting blood sugar levels of diabetic patients This study revealed that only 9.2% of the total sugar levels above 180 mg/dl (table 3). High number of patients with DM had fasting blood sugar percentage (57.7%) of type 1 DM patients had their levels below 140 mg/dl, 55% of all patients had fasting blood sugar levels above 180 mg/dl level, their fasting blood sugar levels in the range of 140-while 32.6% of type 2 DM patients had their fasting 180 mg/dl, while 35.8% had their fasting blood blood sugar levels above 180 mg/dl level. Microvascular complications of DM 41.5% of all diabetic patients suffered from at least one microvascular complication. The most common was retinopathy (seen in 16.2% of the patients), followed by peripheral neuropathy (11.2%), then peripheral neuropathy and retinopathy (6.5%). Most of the complications (87.3%) were seen in patients with type 2 DM. Retinopathy was seen in 13.1% of these patients (table 4). Microvascular complication usually relates to the duration of illness, where it was found that the incidence of the complication increases by increasing the duration of the illness. Diabetic nephropathy took a longer time to develop, where most of the cases were seen after 10 years of the illness (figure 1). Discussion The majority of the diabetic cases in the study belonged to type 2 DM, these results are well correlated with the results of a study done in USA which reported that type 2 diabetes accounts for about 90 to 95 percent of all diagnosed cases of diabetes4. Identical results were reported on a Libyan population in Benghazi (2007), where the majorities (87.2%) of the diabetic patients were of type 25 . 73.4% of all patients had a family history of diabetes. Family history of diabetes has been recognized as an important risk factor of the disease. In the U.S. population, family history of diabetes has a significant independent and graded association with the prevalence of diabetes6. These findings are consistent with a summary review of ten studies performed in various countries, which reported that individuals with a positive family history of diabetes had two to six times the risk of type 2 diabetes, compared with individuals without a family history of the disease7. Moreover, close relative marriage is very common in the Libyan society. It has been suggested that among all demographic and risk factors, the presence of three or more diabetic firstdegree relatives corresponded to the highest diabetes prevalence for diabetes8. This might explains the high percentage of patients with family history of diabetes reported in this study. This association opens the possibility of adding family history to public health strategies in Libya aimed at detecting and preventing the disease at early stages. Obesity is another major problem reported in this study, especially with type 2 female diabetic patients (table 1). The association between obesity and risk of developing diabetes has been well documented in several nations (e.g. China9, USA10, Turkey11 France12 and Italy13). Environments with plentiful food and low physical activity are well suited for the development of obesity and ultimately type 2 diabetes. Previous studies have demonstrated that changes in lifestyle are effective in preventing diabetes and obesity in selected groups of adults who are at high risk14. Therefore, obesity could be a major factor in the development of diabetes mellitus in the Libyan patients that requires intervention by educating diabetic patients of the importance of regulating their diet and the involvement in more physical activity to improve their health style. High percentage of diabetic patients were above 40 years old, where almost all patients with type 2 DM were above 30 years old. This is in accordance with the findings that over 95 percent of persons with type 1 DM develop the disease before the age of 25, while type 2 tend to occur at older age15. The influence of age on the development of diabetes is an international phenomena. In a study done in USA the prevalence of diabetes rose rapidly from a range of 1.4-3% for age category 20-39 years to an average of 17.3-29.3% for age category 60-74 years16. Similar results were reported with other nations17,18. Insulin was given to 38.8% of all diabetic patients, while 35.4% of the patients were treated with oral hypoglycemics. 32.6% of the patients with type 2 DM were treated with insulin (table 2). In the study done in Benghazi (2007), 39.6% of all type 2 diabetic patients were treated with insulin5. In Australia, data show that 96% of type 1 DM and only 6.4% of type 2 DM were treated with insulin. On the other hand, nearly equal percentage were treated with a combination of insulin and oral hypoglycemics (3%), and about 58% of the type 2 diabetic patients were treated with oral hypoglycemics19. In USA, a 2006 study showed that among adults with diagnosed diabetes (type 1 or type 2) 14% take insulin only, 13% take insulin and oral medication, 57% take oral medication only, and 16% do not take either insulin or oral medication4. The high percentage for the use of insulin in type 2 DM in this study might indicate the poor compliance of the patient to therapy with oral hypoglycemics, the condition that will result in poor control and will force the physician to prescribe insulin in order to avoid or delay the appearance of diabetic complications. Most of diabetic patients in this study had fasting blood sugar levels above the international recommended levels in spite of the fact that 38.8% of them were treated with insulin (table 3). The acceptable fasting blood sugar level as it is recommended by the American Diabetes Association and the European Association for the Study of Diabetes is in the range of 70-130 mg/dl20. Three possibilities can be drawn from these results, patients’ incompliance with therapy, patients were not fasting before sampling, or inaccurate measurements of blood glucose levels. The clinical trials, in concert with epidemiological data, support decreasing glycemia as an effective means of reducing longterm microvascular and neuropathic complications20. Further more, other more accurate measures such as postprandial blood sugar and A1C levels should be used as a measure of glycemic control in Libyan patients. 41.5% of all diabetic patients suffered from at least one microvascular complication (retinopathy, peripheral neuropathy or a mixture of neuropathy and retinopathy) (table 4). These microvascular complications were found to be related to the duration of illness where diabetic nephropathy took a longer time to develop (figure 1). This is in agreement with other reports that retinopathy can be detected in nearly every patient after diabetes duration of 20 years21. It was reported that diabetic nephropathy accounts for 19% of end stage renal disease, microalbuminuria which is an early marker of diabetic nephropathy, can be found in 30% of the patients after 10 years of diabetes21. Due to the severity of the diabetic complications many studies regarded that an early intensified antidiabetic treatment is highly important for the prevention of microvascular events. The limitation of this study was the small number of patients involved which should be extended to a larger number of patients. Recommendation A national diabetic policy following the guidelines set by World Health Organization (WHO) is urgently needed. Education and training of the patients and their families about diabetes mellitus are the key steps in improving health outcomes and quality of life. It should focus on self-care behaviors, such as healthy eating, being active, monitoring blood glucose and strictly adhering to treatments. Conclusion This study revealed many important facts related to diabetic patients in the city of Misurata and indicated the need of a national policy about the diseas, that majority of the patients had family history of diabetes. Acknowledgements We are grateful to the staff of the centre for management and treatment of diabetes and endocrine disorders, Misurata – Libya for helping us in the acquisition of data from their patients file. We are also thankful to the patients who were very helpful and understanding. African Health Sciences Vol 12 No 1 March 2012 References
Copyright 2012 - African Health Sciences The following images related to this document are available:Photo images[hs12015t2.jpg] [hs12015t3.jpg] [hs12015t1.jpg] [hs12015t4.jpg] [hs12015f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}