
|
Journal of Indian Association of Pediatric Surgeons
Medknow Publications on behalf of the Indian Association of Pediatric Surgeons
ISSN: 0971-9261 EISSN: 1998-3891
Vol. 10, Num. 1, 2005, pp. 37-40
|
Journal of Indian Association of Pediatric Surgeons, Vol. 10, No. 1, January-March, 2005, pp. 37-40
Original Article
Proximal bowel T-tube drainage and local instillation of N-acetyl cysteine: A modified approach to management of meconium ileus
Bhattacharyaya S., Basu K.S., Samanta N.
Department of Pediatric Surgery, N.R.S. Medical College and Hospital, Kolkata
Correspondence Address:Department of Pediatric Surgery, N.R.S. Medical College and Hospital, Kolkata
E-mail: mimisangha@india.com
Code Number: ip05009
Abstract
Various surgical procedures are described and practiced for operative management of uncomplicated meconium ileus. In our series, we have tried an approach of minimally invasive procedure to minimize the operative stress in already sick neonates.
Ten cases of meconium ileus operated between 01/01/2003 to 21/06/2004 were screened. Three cases presented with complications like peritonitis (2) and volvulus (1) and so were not included in this study. Seven cases were uncomplicated. Out of them three were managed conservatively. Operative management by minilaparotomy - enterotomy and T-tube insertion was done in the remaining four cases, which did not resolve by conservative approach. In this group, patients passed stool by approximately seventh day (range - sixth to eight day). Oral feeds begun on approximately ninth day (range - eighth to tenth day). All four babies survived.
This approach of minilaprotomy, T-tube insertion and N acetyl cysteine instillation, could be of significant benefit in an already sick neonate. Also, T- tube helps in post- operative bowel decompression, distal bowel wash and check dye study.
Key words: Meconium ileus, T- tube drainage, N-acetyl cysteine
INTRODUCTION
Meconium ileus is one of the leading causes of neonatal intestinal obstruction.
Approximately 50% of the disease process present with complications
e.g. volvulus, intestinal atresia or perforation peritonitis. Uncomplicated
meconium ileus is best managed conservatively by bowel wash with or without
fluoroscopic guidance. Substances used are Gastrograffinβ (Meglumine
diatrizoate66% with Sodium diatrizoate 10% with Iodine)
with or without Tween 80β, Tween 80β, N-acetyl cysteine, Conrayβ (Sodium
iothalamate 70% w/v) or Hypaqueβ (Sodium diatrizoate 45% w/v
with Iodine 270 mg/dl). Surgical intervention is reserved only for complications
during the conservative management and for the complicated cases. Surgical
interventions include- resection and enterostomy, or end to back / back
to end anastomosis with creation of stoma or end to end anastomosis with
or without a vent. These are major operative procedures and is likely
to be associated with higher morbidity especially in sick neonates. Thus
less invasive methods have been tried and used in uncomplicated cases
which donot resolve with conservative management. Methods described are
- enterotomy through a purse string suture and prolonged irrigation with
N - acetyl cysteine (3), or irrigation with Gastrograffinβ via the
appendix stump (9), or enterotomy, irrigation and T-tube ileostomy.[1],[3] In
our study, we have used the last option mentioned for a group of neonates
with uncomplicated meconium ileus not resolving by conservative approach.
Materials and Methods
Ten cases of neonatal intestinal obstruction with features suggestive of meconium ileus were admitted between 1/1/03 to 21/6/04. Average age on presentation was 4 days (range 3-5 days). Presenting features were abdominal distention, bilious vomiting and non-passage of meconium. Per rectal examination and bowel wash revealed meconium pellets or small quantity of thick tenacious meconium or meconium plug.
Investigations included: Routine hemogram, serum electrolytes estimation
and roentgenogram of abdomen in erect posture.
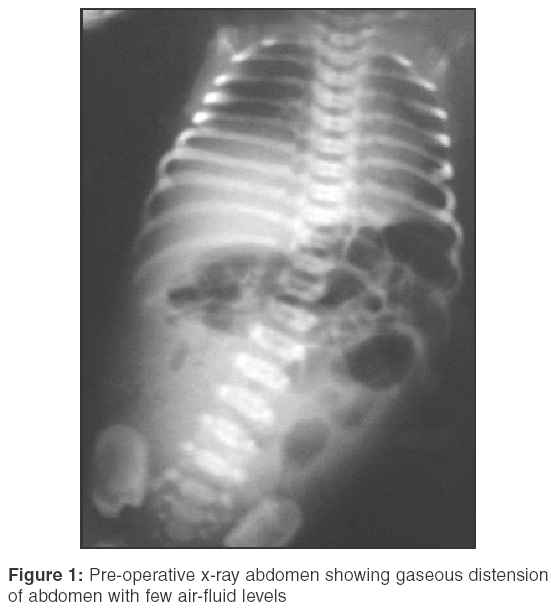
In 7 cases, roentgenogram abdomen revealed gaseous distention of abdomen with
few air-fluid levels (Figure 1).
In the remaining 3 cases roentgenogram showed significant air-fluid levels
in 2 cases and features of perforation peritonitis in 1 case.
Conservative management by bowel wash with normal saline and N- acetyl
cysteine was carried out in 7 cases with features of uncomplicated meconium
ileus, and there was response in 3 cases. Surgical intervention was planned
in the remaining 4 cases by minilaparotomy and T- tube insertion.
Operative procedure
On exploration through right transverse supraumbilical incision
distended small intestine with meconium sludge and pellets packed in
the distal 10-15 cm of ileum along with microcolon was found. No other
features suggestive of complication e.g. volvulus or atresia were found.
Enterotomy was done in the dilated ileum proximal to the part packed
with meconium sludge and pellets, about 15-20 cm from ileo-cecal junction.
Intra operative wash of distal ileum was done with normal saline and
2% N-acetyl cysteine(by diluting available 20% N-acetyl cysteine with sterile water). Enterotomy was closed over No. 12 French Kehr′s T-tube. That part of ileum was fixed to the parieties and the T-tube was brought out through a separate stab incision on the abdominal wall and fixed with skin. (Figure 2).
Post operatively, T-tube was flushed with 5 ml of 2% N-acetyl cysteine thrice daily for approximately 9 days (range of 8-10 days) starting from 1st post operative day.
Results
Patients started passing meconium from approximately 7th (range
5th to 9th) post operative day. The consistency
gradually became softer. In most of the cases, enteral feed could be
started by approximately
8th (range-7th to 10th) post operative day.
Water soluble dye study by 60% urograffin was done through T-tube
on an average 10th post operative day (Figure 3)
and T-tube was removed after confirming free flow of dye distally.
Babies were discharged by an average 11th day.
In one patient the T-tube slipped out on 5th post operative
day, and there was leakage of ileal contents through T-tube insertion
site. Leakage persisted for about 6-7 days. As it was not a major leak,
enteral feeding along with oral antibiotics were continued. Leak subsided
with conservative management.
All the 4 patients have been followed up for approximately 5 months
(range of 4-6 months). Babies have gained weight normally. After
initial period
of breast feeding, weaning was started No history of recurrent respiratory
tract infection has been noted. Cystic fibrosis is not very common
in this part of the country and also due to non-availability of sophisticated
tests, we havenot performed routine screening for cystic fibrosis.
Discussion
The operative management of uncomplicated meconium ileus previously involved resection of the dilated bowel with an enterostomy of Roux-en-Y variety or a primary anastomosis with or without a protective stoma. These procedures would add up to the morbid status of already sick neonates by increasing the operating time, loss of intestine, and problems related to stoma and its care. We are now fully convinced by the fact that grossly dilated completely obstructed bowel can be expected to return to normal once the cause of obstruction has been dealt with.[12] Thus, resection of dilated but viable ileum is not necessary for prompt intestinal function in the neonate.[4] In
about 2/3rd of the uncomplicated cases of meconium ileus therapeutic
enema is the only necessary management. As the mechanical block in removed,
the bowel reverts to normal functions. Various agents are used for therapeutic
enema in uncomplicated meconium ileus e.g. Gastrograffinβ with or without Tween 80β, Tween 80β alone, Hypaqueβ, Conrayβ and
N-acetyl cysteine. In 1964, Mecker and Kincannon reported on the liquefying
effects of N-acetyl cysteine and H2O2 on inspissated meconium causing intestinal obstruction in 9 new born infants.[13] This
was probably the 1st reported use of N-acetyl cystine for meconium ileus.
Subsequently different other authors reported the use of N-acetyl cysteine
for such cases and the concentration to be used has been standardised
to 2-4%.
In cases unrelieved by non operative management, enterotomy and irrigation was described first by Hiatt and Wilson.[14] Subsequently Kalayoglu et al in 1971 reported successful management of 24 neonates with enterotomy and irrigation with H2O2 and N-acetyl cysteine.[15] Venugopal and Shandling has a similar series with successful management of 11 out of 12 cases with the above method.[3] Enterotomy and irrigation has been used as operative procedure by several others.7],10],13] A purse string suture is placed on the antimesentric border of the dilated ileum near the junction of dilated gut with narrowed gut and a soft catheter is inserted through enterotomy. The lumen is gently irrigated and the solution manually mixed with the meconium sludge and pellets.
The thick meconium is then either removed through the enterotomy or flushed into the colon. Fitzgerald in his series of 3 cases used appendix stump for the intra operative irrigation.[9] The only disadvantage of the above procedure is the operative time needed for prolonged irrigation.
O′Neill et al in 1970 reported the use of a tube enterostomy placed at the junction of the proximal distended bowel and distal small caliber bowel.[16]
In our study, we have used a T-tube instead of a simple tube. T-tube helps in decompression of proximal bowel besides the advantage of post operative irrigation. Since T-tube provides the privilege of performing post-operative wash, a thorough intra-operative wash can be avoided, thus saving some precious operative time A post operative dye study through T-tube helps to confirm the patency of the distal gut. With the use of pancreatic enzyme irrigation, the tenacious meconium in these patients can be rapidly liquefied and expelled per rectally and the necessity of mechanical removal during the operative procedure can be avoided[4]
Miller et al in
his series of 5 patients confirmed the advantage of this technique over
other operative procedures in the management of uncomplicated meconium
ileus not responding to decompression by gastrograffinβ enema[8]
The operative procedure requires less time compared to the other methods, and the T-tube helps in post operative decompression of the proximal bowel, irrigation of the distal bowel and finally provides the opportunity of performing postoperative dye study to confirm the clearance. Thus, T-tube ileostomy followed by post operative irrigation with N-acetyl cysteine is an effective and safe procedure for uncomplicated cases of meconium ileus that donot respond to conservative approach.
References
| 1. | Mak GZ, Harberg FJ, Hiatt P, Deaton A, Calhoon R, Brandt ML. T-tube ileostomy for meconium ileus: Four decades of experience. J Pediatr Surg 2000;35:349-52. Back to cited text no. 1 [PUBMED] [FULLTEXT] |
| 2. | Wit J, Sellin S, Degenhardt P, Scholz M, Mau H. Is the Bishop - koop anastomosis in treatment of neonatal ileus still current? Chirurg 2000;71:307-10. Back to cited text no. 2 |
| 3. | Venugopal S, Shandling B. Meconium ileus: Laparotomy without resection, anastomosis or enterostomy. J Pediatr Surg 1979;14:715-8. Back to cited text no. 3 [PUBMED] |
| 4. | Harberg FJ, Senekjian EK, PoKorny WJ. Treatment of uncomplicated meconium ileus via T-tube ileostomy. J Pediatr Surg 1981;16:61-3. Back to cited text no. 4 [PUBMED] |
| 5. | Nguyen LT, Youssef S, Guttman FM, Laberge JM, Albert D, Doody D. Meconium ileus: Is a stoma necessary? J Pediatr Surg 1986;21:766-8. Back to cited text no. 5 [PUBMED] |
| 6. | Ein SH, Shandling B, Reilly BJ, Stephens CA. Bowel perforation with non operative treatment of meconium ileus. J Pediatr Surg 1987;22:146- Back to cited text no. 6 [PUBMED] |
| 7. | Caniano DA, Beaver BL. Meconium ileus: A fifteen years experience with 42 neonates. Surg 1987;102:699-703. Back to cited text no. 7 [PUBMED] |
| 8. | Millar AJ, Rode H, Cywes S. Management of uncomplicated meconium ileus with T-tube ilesetomy. Arch Dis Child 1988;63:309-10. Back to cited text no. 8 [PUBMED] |
| 9. | Fitzgerald R, Conlon K. Use of the appendix stump in the treatment of meconium ileus. J Pediatr Surg 1989;24:899-900. Back to cited text no. 9 [PUBMED] |
| 10. | Rescorla FJ, Grosfeld JL. Contemporary Management of meconium ileus. World J Surg 1993;17:318-25. Back to cited text no. 10 [PUBMED] |
| 11. | Weber TR, Tracy TF Jr, Silen ML, Powell MA. Enterostomy and its closure in newborns. Arch Surg 1995;130:534-7. Back to cited text no. 11 [PUBMED] |
| 12. | Noblett HR. Treatment of uncomplicated meconium ileus by Gastrograffinβ enema: A preliminary report. J Pediatr Surg 1969;4:1909-7. Back to cited text no. 12 |
| 13. | Meeker IA Jr, Kincannon WN. Acetyl cysteine used to liquify inspissated meconium causing intestinal obstruction in the new born. Surgery 1964;56:419-25. Back to cited text no. 13 |
| 14. | Hiatt RB, Wilson PE. Celiac Syndrome: Therapy of meconium ileus: Report of eight cases with a review of the literature, Surg Gynecol Obstet 1948;87:317. Back to cited text no. 14 |
| 15. | Kalayoglu M, et al : Meconium ileus: A critical review of treatment and eventual prognosis. J Pediatr Surg 1971;6:290-300. Back to cited text no. 15 |
| 16. | O' Neill JA Jr, Grosfeld JL, Boles ET Jr, Clatworthy HW Jr. Surgical treatment of meconium ileus, Am J Surg 1970;119:99-105. Back to cited text no. 16 |
Copyright 2005 - Journal of Indian Association of Pediatric Surgeons
The following images related to this document are available:
Photo images
[ip05009f3.jpg]
[ip05009f2.jpg]
[ip05009f1.jpg]
|

{kind=link}
{kind=link}
{kind=link}