 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
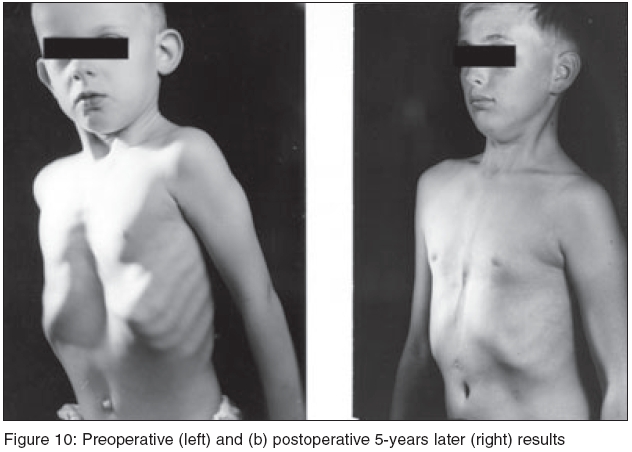
Journal of Indian Association of Pediatric Surgeons, Vol. 10, No. 3, July-September, 2005, pp. 147-157 Review Articles Pectus excavatum, pectus carinatum and other forms of thoracic deformities Saxena AmulyaK Department of Pediatric Surgical University Medical Centre, Münster, Germany Code Number: jb05037 Abstract This review article covers the spectrum of congenital thoracic wall deformities along with their historical background. Willital's classification divides these deformities into 11 types - funnel chest (4 types), pigeon chest (4 types), and combination of funnel and pigeon chest, chest wall aplasia and cleft sternum. Records of patients at our center comprised 90% depression deformities, 6% protrusion deformities, 3% combined depression-protrusion deformities and 1% other forms. Mild forms of abnormalities warrant the wait- and-watch approach during the first 4-5 years. The deformities manifest primarily during the pubertal spurt often with rapid progression with subjective complaints like dyspnea, cardiac dysthesia, limited work performance and secondary changes. Operative correction in young adults is more favorable in mild cases. The Willital technique has been the standard technique for the correction of pectus excavatum, pectus carinatum and other combined forms of deformities at our center with excellent long term results. The Nuss procedure and the Pectus Less Invasive Extrapleural Repair (PLIER) technique for pectus excavatum and pectus carinatum have also been described in this article. Surgical correction for Poland's syndrome is reserved for patients with severe aplasia of the ribs with major depression deformity. Sternal defects including various types of ectopia cordis are discussed. Even after surgical correction, there is significant reduction in the total capacity and inspiratory vital capacity of the lungs, probably a result of the decreased compliance of the chest wall. However, the efficiency of breathing at maximal exercise improves significantly after operation. Keywords: Pectus excavatum, Pectus carinatum, Congenital chest wall deformities Congenital thoracic wall deformities represent a spectrum of musculo-skeletal disorders of the anterior chest wall. Most of these deformities fortunately are not life-threatening and do not manifest in severe functional pathophysiology of the thoracic organs. The management of these deformities, however, has gained more importance in the past decade because of the increased participation in competitive school sports as well as athletics, and the changing trends in the world of fashion which expose more of the chest to the public view. It is important to note that, although thoracic wall deformities do not arouse the sympathy generated by limb or cranial anomalies, children with such deformities are viewed with curiosity by their classmates and are often confronted by teasing remarks. Except for severe chest wall deformities, it is generally extremely difficult to predict the course of progression after the deformities have been discovered in early infancy. Therefore, mild forms of abnormalities warrant the wait- and-watch approach during the first 4-5 years before operative management could be considered. In mild cases, the dormant deformity sometimes becomes accentuated during adolescent growth. Since, the deformities can also manifest frequently primarily during the pubertal spurt often with rapid progression, operative correction in young adults is more favorable in mild cases. The wait-and-watch approach must consider the vertebral anomalies such as scoliosis that may significantly result or affect the secondary deformities of the thoracic cage. Cardiopulmonary effects Chest wall depression is better tolerated in infancy, however many older children report subjective complaints such as dyspnea, cardiac dysthesia and limited work performance. Chest wall depression results in a variable displacement of the heart to the left and could be associated with significant rotation. This is well documented by CT scans of the thorax that demonstrate the degree of cardiac compression resulting from the sternum and costal cartilages. Although, surgical correction has been performed in many centers mainly for esthetic and psychological reasons, however, compression and secondary changes of the intrathroracic organs have been indications for surgery.[1] [Figure - 1] Many individual patients reported with specific cardiac problems, such as supraventricular tachycardias and recurrent heart failure, were relieved by correction of the depressed sternum. Mechanical factors such as cardiac displacement due to the deformity are furthermore responsible for the functional disturbances of the right and left sides of the heart in systole and diastole. This has been attributed to be more a disorder of compliance of the right side of the heart than the output of the ventricle. Decreased right ventricle filling due to impaired function of the right atrium is also responsible for the reduced stroke volume during exercise.[2] Preoperative echocardiographic and Doppler findings have also correlated well with the extent of cardiac displacement.[3] A significant increase in the cardiac index after operation is evident when patients performed exercises in sitting position, presumably on the basis of an increased stroke volume. A decrease in the heart rate at any given work performance after operation, evident as the improvement in exercise capacity, is due to the result of an increase in cardiac stroke volume and could explain the subjective circulatory stabilization experienced by the patients. Restrictive impairment of pulmonary function, expressed by reduced total lung capacity and inspiratory vital capacity is found in patients with funnel chest [4],[5],[6] although normal functions have also been observed.[7],[8] Even after surgical correction of the deformity there is a significant reduction in the total capacity and inspiratory vital capacity of the lungs, probably a result of the decreased compliance of the chest wall.[9],[10] However, the efficiency of breathing (ratio of tidal volume / inspiratory vital capacity) at maximal exercise improves significantly after operation.[2] Classification Patients with chest wall deformities are best graded according to the Willital′s classification, which is based on morphologic findings of the thorax. [Figure - 2] This classification divides congenital chest wall deformities into 11 types - funnel chest (4 types), pigeon chest (4 types), combination of funnel and pigeon chest, chest wall aplasia and cleft sternum [Table - 1].[11] Since most of the centers today employ metal struts for the correction of this deformity, this classification allows assessment of the operation technique with regards to the location of implantation of the metal struts, as well as the determination of the number of struts to be used for internal stabilization of the chest wall.[12] Records of patients with thoracic wall deformities at our medical center have shown 90% with depression deformities, 6% with protrusion deformities, 3% with combined depression-protrusion deformities, and 1% with other forms.Pectus Excavatum Historical Background of Surgical Repair Clinical relevance Pectus Carinatum Historical Background of Surgical RepairPectus carinatum (pigeon chest), a protrusion deformity is the second most common malformation of the anterior chest wall. Ravitch in 1952 was the first to suggest that surgical correction was the only effective method for the treatment of this deformity. He surgically corrected the chondromanubrial prominence by resecting the multiple deformed costal cartilages and performing a double osteotomy.[24] Later on, Lester in 1953 performed a repair involving resection of the anterior part of the sternum, but abandoned this approach due to unsatisfactory results. He then reported a second less radical technique which involved subperiosteal resection of the lower body of the sternum and sternal ends of the costal cartilages.[25] Chin in 1957 and Brodkin in 1958 employed an operative procedure which used the traction effect of the rectus muscles to relocate and maintain the sternum in a corrected position.[26],[27] This method was further modified by Howard who preferred the radical resection of cartilages and a sternal osteotomy.[28] Later, in 1960, Ravitch reported another surgical procedure that left the sternum alone, and involved the resection of the affected costal cartilages along with the shortening of perichondrial strips with reefing sutures.[29] In 1963, Ramsay utilized a rectal muscle flap to fill the lateral defects resulting from the protrusion without altering the position of the sternum or resecting the deformed costal cartilages.[30] Also in 1963, Robicsek reported a technique that involved subperichondrial resection of the deformed lateral asymmetric costal cartilages, transverse sternal displacement, and resection of the protruding lower portion of the sternum along with the reattachment of the xiphoid and rectus muscles to the new lower margin of the sternum.[31] Welch in 1973 and Pickard in 1979 reported techniques which were similar and involved costal cartilage resection and sternal osteotomy.[32],[33] Clinical relevance Pectus carinatum represents an array of abnormal development of the anterior chest wall. In our single center surgical experience it constitutes 12% patients operated upon with anterior chest wall deformities with a 2:1 male-female predominance. Although the pathogenesis of pigeon chest is not exactly defined, excessive overgrowth of costal cartilages has been implicated in the etiology of both, pectus excavatum as well as pectus carinatum.[34] The delayed clinical presentation of pectus carinatum when compared to pectus excavatum, may be due to the fact that the protruding infantile abdomen accentuates pectus excavatum in early childhood and recession of the abdominal contour which occurs in the later years emphasizes the protrusion defect in early adolescence. Musculoskeletal abnormalities, most frequently scoliosis, are associated with pectus carinatum, and may not require surgical correction.[35] The severity of the deformity is extremely variable. Surgical correction has been performed mainly for esthetic and psychological reasons; however, displacement and secondary changes of the intrathroracic organs have been indications for surgery.Surgical Technique For Pectus Excavtaum & Pectus Carinatum The Willital technique has been the standard technique for the correction of pectus excavatum, pectus carinatum and other combined forms of protrusion-depression combined deformities at our center with excellent long term results. Using this technique, repair is performed using a standard method of double bilateral chondrotomy parasternally and at points of transition to normal ribs. This is followed by detorsion of the sternum, retrosternal mobilization, correction of the inverted ribs and stabilization of the displaced sternum with one transternal and two bilateral parasternal metal struts. The technical steps have been elaborated below to explain this surgical procedure. A vertical midline incision is made in boys; otherwise in girls, a submammary incision that is curved upward at the midpoint (over the deepest point of the sternal defect) is preferred, thus avoiding the complication of breast deformity and impaired breast development.[36] [Figure - 5] In the incision, skin, fat and pectoral muscles are reflected in a single flap and the entire dissection is performed with a needle-tipped electrocautery. The pectoral muscles are severed from its insertion at the edge of the sternum and costal cartilages to expose the entire impression of the deformity, generally formed by 5-8 pairs of ribs (third to tenth rib). When the deformed costal cartilages have been completely exposed, the perichondrium is incised with the needle-tip cautery in form of an H [Figure - 6]. The subperichondrial dissection is carried out with small, sharp periosteal elevators and the perichondrium is pealed away from the underlying cartilage [Figure - 7]. The deformed costal cartilages are resected parasternally from their junction with the rib to within 1 cm of the sternum as well as at the level of transition to the normal ribs, leaving the uppermost normal cartilages intact [Figure - 8]. The attachment of the rectus muscle to the sternum is severed, and the sternum is elevated with a Kocher clamp and dissected free from the anterior mediastinal tissue after retrosternal mobilization. A partial transverse sternal wedge osteotomy is performed at the Angle of Ludovici. Once the sternum is dissected free as described, a perforated steel strut is then passed trans-sternally, with its edges resting anteriorly on the ribs. The strut must be bent in such a way so that it fits the thoracic wall perfectly at the edge of the impression. Two parasternal metal struts are also employed, with the points of fixation being the second rib and the lowest end of the rib cage [Figure - 9]. The transsternal strut is fixed to the two parasternal struts with stainless steel wires for additional support. The two parasternal struts also provide anchorage to the completely mobile chest segments, which were formed as a result of double bilateral chondrotomy. Heavy resorbable suture material is then used to close the sternal osteotomy as well as to secure the struts to the chest wall. Two single limb chest tubes are placed in parasternal positions at the level of the highest costal cartilage resection. The pectoral muscle flaps and the severed rectus muscles are then sutured and fixed to the sternum. The overlying subcutaneous and cutaneous structures are finally united in the conventional manner to restore the normal chest wall anatomy. Perioperative antibiotic therapy is administered; with ceftriaxon being the drug of choice. All patients are also administered strong analgesics for first 24-72 hours. The chest tubes are generally removed on the third day or when the drainage is < 25ml for a twelve-hour shift. Wound infections are rare and the patients are mobilized after chest tube removal. On the fourth day pulmonary exercises are commenced and are continued for a period of three weeks. At the time of discharge patients are advised to avoid body contact sports until the struts have been removed. The struts are removed after a period of 12 months in patients > 12years, but are retained for 15-24 months in younger children, so as to stabilize the thorax that is still under the growth spurt. Stainless steel alloy implants have been accepted as the standard prosthetic implant material for the operative treatment of thoracic wall deformities. Allergy to stainless steel alloy implants is seldom experienced in patients, but may have fatal outcomes if not detected prior to surgery. Patients with allergy to nickel, an element that is present in stainless steel alloy implants, have been managed using titanium implants using polyethyleneterphtalate sutures which exhibit fixation capabilities of similar magnitude to 20-gauge stainless steel wires to secure the sternum and ribs.[37] Results Repairs are generally completed with an extremely limited number of mild complications like pneumothorax, pleura effusions or wound infections. Cardiopulmonary injuries are rare and blood transfusions are seldom required. Good long term results have been reported worldwide after the surgical correction of funnel chest deformities with a relatively low recurrence rate of 2-5%. Lower rates of recurrence have been observed also in many long-term studies after the correction of funnel chest.[1],[38],[39],[40],[41] Irrespective of the technique, we consider the main reasons for recurrence are (a) inadequate mobilization of the depressed chest wall (b) unstable fixation of the mobilized chest wall and (c) no or inadequate remodeling of the lowest parts of the deformed ribs.[42] Complete exposure of sternum and ribs is necessary for satisfactory results as it allows complete intraoperative assessment of the deformity and is of significant importance in patients > 15 years of age who may require an additional transsternal strut because of the extensive area of sternal depression.[10] This also allows placement of struts and stainless steel wires under complete vision and avoids serious complications such as cardiac perforation.[43]Minimal Invasive Repair For Pectus Excavatum Minimal invasive repair of Pectus Excavatum was introduced by Donald Nuss and this procedure is more commonly known as the "Nuss Procedure".[44] This procedure opts for a minimal invasive route to correct the deformity without resection of the deformed cartilages. Basically, it involves minimal bilateral skin incision of 2-3 cm in the anterior axillary line to gain access to the thorax. An introducer , which is a long blunt rod, is pushed through to the other side of the chest. A cotton tape is then tied to the eyelet at the end of the introducer. The introducer is pulled back through along with the cotton tape. A metal bar (Lorenz Surgical, Inc, Jacksonville, FL, USA), is bent to conform to the size and the desired thorax form. The cotton tape is tied to the curved pectus bar. The bar is then pushed through the tunnel, curved side down. The tape is pulled from the other side to help move the bar along. The bar flipper , a cranklike tool that fits on to the end of the bar, is used to turn the bar. The curved flipped bar pushes the funnel to correct the deformity. [Figure - 11] The bar is further stabilized with metal plates, metal wires or PDS sutures on one or both sides to prevent dislocation. The skin incisions are closed and no drains are employed. With the advent of thoracoscopy, introduction of the bar has become safer and serious complications such as cardiac injury have been avoided. In case of severe deformities and asymmetric forms of pectus excavatum additional bars can be introduced in the similar way as described above. Over-correction of the pectus deformity should be generally avoided, since placement of over-corrected bars can cause excessive displacement of the sterum and a pectus carinatum type deformity. The bars are left generally for a period of 3 years in position after which they are removed. [Figure- 10]"Plier" Pectus Less Invasive Extrapleural Repair The Pectus Less Invasive Extrapleural Repair "PLIER" technique is a less radical method developed to operatively manage pectus excavatum as well as pectus carinatum and to avoid the possible cardiac injury that may occur by the minimal invasive technique.[45] The PLIER technique involves small skin incisions of 7-10 cm after which the musculo-cutaneous flap is mobilized. After dissection of the pectus muscles, an extra-pleural space is created with careful digital mobilization.[46] Bilateral parasternal chondrotomy is performed along with chondrotomy at the point of rib culmination. A trans-sternal as well as two longitudinal struts are placed to stabilize the flail thoracic segments. The procedure is completed without placement of chest tubes or suction drains.[47] Postoperative pain is significantly lower in these patients and early mobilization is possible. The PLIER method has been developed to approach the (a) pectus carinatum and (b) severe asymmetric pectus excavatum, both deformities that are difficult or not possible to correct using the minimal invasive Nuss procedure. [48] Our initial experience with PLIER for pectus repair has shown excellent results during the follow-up examinations [Figure - 12].Poland′s Syndrome Poland′s syndrome is a spectrum of anomalies that include the absence of the pectoralis major and minor muscles along with a complex of hand anomalies including syndactyly, brachydactyly or ectrodactyly, deformed or absent ribs, absence of axillary hair and decreased amount of subcutaneous fat. Lallemand in 1826 and Froriep in 1839 initially descried this syndrome, however it was Poland, an English medical student, in 1841 who published a partial description observed during his anatomic dissection. [49],[50],[51] It was however Thomson in 1895 who elaborately described the full spectrum of the deformity.[52] The extent and the severity of involvement of the anomalies is variable and its presentation can differ in the affected patients. Poland′s syndrome is seldom familial and is associated with a sporadic occurrence in approximately 1:30000 live births.[53],[54] The exact etiology of Poland′s syndrome is however not yet established. It is however thought that abnormal migration of the embryonic tissue forming the pectus muscle, hypoplasia of the subclavian artery or intrauterine injuries may be responsible. Surgical correction for patients with Poland′s syndrome is reserved for patients with severe aplasia of the ribs with a major depression deformity. Several techniques such as split rib grafts with Teflon felt and latissimus dorsi muscle flaps with placement of rib grafts have been employed for the correction of the deformed ribs.[55],[56],[57] We prefer to use the surgical technique described previously, for the correction of the partially hypoplastic thoracic cage with excellent results. Breast reconstruction is required in most girls but it is best delayed until late puberty to achieve optimal reconstructive results compared to the growth of the contralateral breast. Most of the surgeons prefer the reconstruction with latissimus dori flaps, however atrophy of flaps with time has been observed. Prosthetic implants have also been employed with mixed results as to their complete success reported. It is of paramount importance to discuss the expectations of the patients and the parents prior to the onset of surgical management to achieve acceptable results. Sternal Defects These defects constitute a broad spectrum of rather rare deformities of the sternum and heart. While the specific cause is yet unexplained, a partial or complete failure of fusion is responsible for the defects that occur. Cardiac pulsations are quite prominent with each type of cleft sternum, suggesting that the heart is partially outside the chest wall (ectopia cordis) in true cases. Associated cardiac defects and multiple anomalies in other body regions usually preclude survival. In 1818 Weese provide the first anatomic classification of the defects. Later on Roth in 1939, Shao-tsu in 1957 and Cantrell in 1958 provided further classifications of sternal defects. Review of the medical literature on this topic provides four types of sternal defects which are largely based on the tissue coverage of the heart.Thoracic Ectopia Cordis This type of sternal defect constitutes a completely open heart with no overlying somatic structures. There open heart is found to be associated with intrinsic cardiac anomalies. The sternum is generally fused cranially however entire split sternum is rare. The pathology is further associated with a lack of midline somatic tissues and a smaller than normal thoracic cavity in the affected infants. Upper abdominal defects such as rectus diastases or omphalocele are frequent but are rarely associated with the eventration of the abdominal viscera. The first attempted repair of ectopia cordis was performed in 1925 by Cutler and Wilens, however, in 1975 it was Knoop who performed the first successful repair. [58],[59] Skin flap coverage had been since used in a two stage reconstruction for the management of thoracic ectopia cordis. However, successful one staged correction has been reported by Amato who performed a construction of the partial anterior thoracic cavity surrounding the heart, but however avoided the return of the heart to its orthotopic location. [60] The successful repair of such anomalies is dictated by the presence and the severity of the intrinsic cardiac anomalies rather than the type of surgical approach itself. There have been no recent advancements or successes reported in the management from the surgical point of view, however advances in fetal ultrasound techniques have aided in the early recognition of the deformity and termination of the fetus in pregnancy. Cervical Ectopia Cordis Cervical ectopia cordis occurs rather infrequently when compared to thoracic ectopia cordis. The patients present with cranial displacement of the heart and the fusion of the apex of the heart and the mouth of the cleft. Several craniofacial anomalies frequently accompany cervical ectopia cordis. Unfortunately these groups of patients face the same fate of morbidity and mortality as those with thoracic ectopia cordis. No successful management or survivors with this anomaly have been reported to date. Thoracoabdominal Ectopia Cordis Syndromes of cardiac and parietal anomalies are generally a part of the defect in the distal closure of the sternum. This syndrome is referred commonly to as a pentology with the following associated anomalies: (a) distal cleft sternum, (b) ventral defect of the anterior abdominal wall that may be a true omphalocele, (c) pericardiopleural communication through an inferior pericardial defect, (d) anterior diaphragmatic defect, and (e) congenital cardiac defect generally in the form of tetralogy of Fallot. It is important to note that these clefts may also occur without the full syndrome. In this defect the heart lacks the severe anterior rotation as seen in thoracic ectopia cordis and is covered by a thin membrane or skin overlying the distal cleft sternum. The position of the heart may also vary from lying in the thoracic cavity to an extreme localization entirely within the abdominal cavity. An interesting finding in this anomaly is the diverticula of the left ventricle which quite frequently protrudes through the diaphragmatic and pericardial defect into the abdominal cavity. The operative correction of the cleft sternum and associated defects require a staged approach, with priority given to the management of the severe defects. The general approach however would most likely mandate primary correction of the omphalocele with a delayed approach to the treatment of the cardiac defect. Advances and experience gained in pediatric cardiac surgery have decreased the morbidity and mortality of these anomalies. Early repair of the defect provides a better opportunity for the direct closure of the sternal defect with the attachment of the diaphragm. Successful operative outcomes and long-term survival are better when compared to thoracic ectopia cordis. Cleft or bifid sternum This is the least severe of the anomaly of the sternum represented by a partial or complete sternal cleft. Most cases however involve the upper part of the sternum and manubrium with an intact xiphoid or intact lower third of the body of the sternum. The heart in these patients is orthotopically located with an intact pericardium along with an intact skin covering. Intrinsic cardiac defects are generally extremely rare. Also, clinically, the patients are asymptomatic and the surgical repair is directed to render protection to the heart. Surgical repair is recommended in infancy within the first 3 months of life when the chest wall is most flexible and primary closure is accomplished without difficulty. Modifications of techniques, with the basic principle of bilateral oblique incision through the costal cartilages to produce greater length to allow midline approximation of the longitudinal sternal ends, lateral cartilage division and medial relocation to close the defect as well as the utilization of prosthetic materials, have been successfully employed for the closure of this defect.References
Copyright 2005 - Journal of Indian Association of Pediatric Surgeons The following images related to this document are available:Photo images[ip05037f10.jpg] [ip05037t1.jpg] [ip05037f9.jpg] [ip05037f4.jpg] [ip05037f7.jpg] [ip05037f8.jpg] [ip05037f1.jpg] [ip05037f12.jpg] [ip05037f3.jpg] [ip05037f11.jpg] [ip05037f6.jpg] [ip05037f2.jpg] [ip05037f5.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}