 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Indian Association of Pediatric Surgeons, Vol. 10, No. 4, October-December, 2005, pp. 229-236 Review Articles Voiding dysfunction - A review Sripathi V Department of Pediatric Surgery and Pediatric Urology, SMF Children's Hospital, Anna Nagar, Chennai and Apollo Hospitals, Greams Road, Chennai Code Number: ip05055 Abstract In a child who is toilet trained the sudden onset of daytime wetting with frequency or urgency is alarming to the parents. Initially this subject was subdivided into a number of descriptive clinical conditions which led to a lot of confusion in recognition and management. Subsequently, the term elimination dysfunction was coined by Stephen Koff to emphasise the association between recurrent urinary infection, wetting, constipation and bladder overactivity. From a urodynamic point of view, in voiding dysfunction, there is either detrusor overactivity during bladder filling or dyssynergic action between the detrusor and the external sphincter during voiding. Identifying a given condition as a 'filling phase dysfunction' or 'voiding phase dysfunction' helps to provide appropriate therapy. Objective clinical criteria should be used to define voiding dysfunction. These include bladder wall thickening, large capacity bladder and infrequent voiding, bladder trabeculation and spinning top deformity of the urethra and a clinically demonstrated Vincent's curtsy. The recognition and treatment of constipation is central to the adequate treatment of voiding dysfunction. Transcutaneous electric nerve stimuation for the treatment of detrusor overactivity, biofeedback with uroflow EMG to correct dyssynergic voiding, and behavioral therapy all serve to correct voiding dysfunction in its early stages. In established neurogenic bladder disease the use of Botulinum Toxin A injections into the detrusor or the external sphincter may help in restoring continence especially in those refractory to drug therapy. However in those children in whom the upper tracts are threatened, augmentation of the bladder may still be needed.Keywords: Dysfunctional voiding in children, Detrusor Sphincter Dyssynergia, Constipation, Dysfunctional Elimination Syndrome Dysfunctional voiding is a ubiquitous disorder in children. It is estimated that 15% of 6 year olds suffer from this condition.[1] The recognition and management of voiding dysfunction is of utmost importance because if neglected upper tract changes and renal failure will ensue in these children. Phases in the development of bladder control Bladder functional development proceeds in fairly well defined stages. The newborn voids about 20 times a day. As he becomes older, the frequency comes down to about 11 times at two years of age. This decrease is accompanied by an increase in the volume of every void. There is a gradual increase in bladder capacity from about 1-2 ounces in the newborn period to an adult capacity at 12 years of age. As a rule of thumb the increase in bladder capacity is one ounce per year of age. At three years of age the striated urethral sphincter comes under voluntary control. The initiation and termination of voiding now becomes volitional. This is ′toilet training′as is conventionally known. The final phase of micturition control is at four years of age when the sacral micturition reflex arc is brought under cortical control. This means the cerebral cortex is able to control the detrusor by initiating or inhibiting a contraction at any given volume. Definition of voiding dysfunction Any functional disturbance in voiding after completion of toilet training
can be called ′dysfunctional voiding′. Voiding dysfunction means any abnormal holding and disturbed voiding pattern seen in a child without anatomical or neurological disease. These definitions cover a wide group of diverse conditions such as: Types of voiding dysfunction In spite of the bewildering variants enumerated above, voiding dysfunction can be simplified into two types: Filling phase dysfunction A forceful detrusor contraction forces urine into the urethra. This is squeezed back into the bladder by a strong contraction of the urethral sphincter. Organisms colonizing the perineum are also taken into the bladder thus initiating a urinary infection. Voiding phase dysfunction Evolution of voiding dysfunction The purge urge syndrome is believed to be due to immaturity of cortical control over the detrusor. Voiding phase dysfunction is believed to be acquired due to habitual postponement of voiding and defecation. Dysfunctional Elimination Syndrome (DES) This term was coined by Stephen Koff to emphasize the association between severe idiopathic constipation, wetting, bladder instability and recurrent urinary infections.[3] Constipation and urinary infections are closely related because the loaded colon presses on the bladder and: In addition encopresis selects uropathogenic
E.Coli in the perineum leading to severe urinary infections. Recognising voiding dysfunction All children with voiding dysfunction present with wetting and / or soiling. Any three of the following six parameters signify presence of voiding dysfunction:[4]
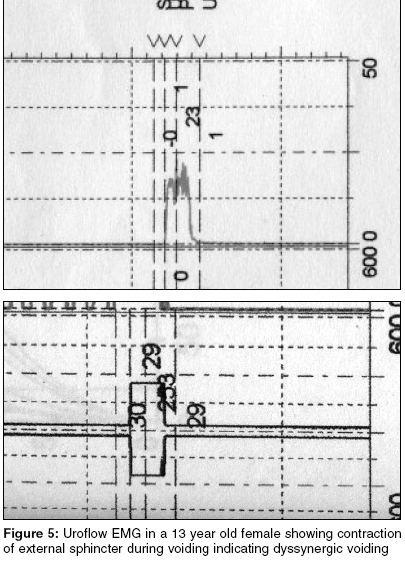
To this can be added: Investigations in voiding dysfunction The classic investigations in urinary infections include renal ultrasound, urine culture and sensitivity, micturating cystogram and DMSA. To this would be added cystometry to diagnose bladder overactivity (filling phase dysfunction) and uroflow EMG to diagnose dyssynergic voiding (voiding phase dysfunction). In uroflow EMG, electrodes are placed in the perineum to pick up activity from the pelvic floor. In a child with voiding phase dysfunction there is intense pelvic floor activity signifying that the urethral sphincter is contracting during voiding. This modality can be used repeatedly to monitor progress of treatment and being non invasive is well accepted by children [Figure - 5]. Treatment of voiding dysfunction This can be divided into the following segments:
Diagnosis and Treatment of Constipation Constipation is common, not life threatening and needs to be treated in a sustained manner. To begin with it will be useful to define constipation using objective criteria. The following clinical symptoms alone or in combination denote constipation:[7] Approximately one-third of constipated children have urinary disorders and one-third of children with urinary infection have constipation.[8],[9] Thus in any child with wetting and urinary infection, treatment of constipation will alleviate urinary symptoms. Treatment of constipation Behavioral changes Diet Fluid Posture Medical Treatment of Intractable Constipation Stage I Stage II This stage of stool softening needs to be continued for a period of at least 2-3 months to get a lasting effect. The end point will be regular toileting, absence of fear and the stools will be soft or even runny in consistency. Dysfunctional Elimination Syndrome (DES) and vesico-ureteric reflux In a study of 143 children with primary VUR, 43 showed evidence of DES. These children had breakthrough infections three times more commonly than the others and unsuccessful outcome following surgery was only in the DES group.[3] This underscores the importance of identifying and treating DES in children with ′primary VUR′. In a multivariate analysis of 2759 children treated in a referral practice an attempt was made to quantify the relationship between DES and VUR. Girls were found to have a higher incidence of DES and VUR when compared to boys. UTI was particularly more common in those children with DES.[4] Biofeedback 1. Transcutaneous Electric Nerve Stimulation (TENS) Alternating pulses at frequencies of 5-10 Hz over 15 minutes is very effective in reducing detrusor overactivity. An increase in frequency to 25-50 Hz enhances detrusor contractility while frequencies of 35 - 50 Hz increase pelvic skeletal muscle contractility as well. The pulse width is usually set at 0.2-0.5 ms. The only side effects reported are skin irritation or mild sensory deficit. Low cost TENS apparatus are freely available in our country and the physiotherapist is quite comfortable in teaching parents how to apply the electrodes and how to manage the therapy. At the same time they also teach the children how to relax the pelvic floor or in those with poor tone exercises to strengthen the pelvic muscles are also taught. TENS therapy needs to be done for at least three months to six months for a substantial benefit. Rrecurrence is common once the therapy is discontinued.[6]
2. Uroflow EMG
3. Rectal probes
4. Intravesical transurethral bladder stimulation Newer advances in drug therapy Oxybutinin has been the standard antimuscarinic drug in the treatment of the overactive bladder. The clinical efficacy of the drug depends on receptor affinity, pharmacokinetics and specificity for the bladder. The effectiveness of the drug is measured by receptor specificity and efficacy to side effect ratio. Oxybutinin is non selective but tolterodine is more bladder specific (less effect on salivary glands) and therefore has a better efficacy to side effect ratio. Furthermore since oxybutinin penetrates the blood brain barrier, it is believed to induce central side effects and impair cognitive function. Solifenacin, the latest molecule, is a selective M3 muscarinic receptor antagonist. This drug has less incidence of dry mouth when compared to tolterodine because of its better bladder selectivity.[13] Oxybutinin when administered intravesically is found to have less systemic side effects. In addition to its antimuscarinic effects it also exhibits local anesthetic properties. This mode of administration is particularly effective for those children who have intolerable side effects on oral administration of the drug. Botulinum A toxin is a presynaptic neuromuscular blocking agent which induces selective and reversible muscle weakness upto several months following intramuscular injection of small quantities. The use of Botox A has been evaluated in children with detrusor overactivity not responsive to orally administered agents, and in whom high bladder pressures threaten the upper tracts. Another indication for Botox A is intrasphincteric injection in those with severe Detrusor Sphincter Dyssynergia (DSD).[14] Injection into the bladder muscle is done either with a metal needle or flexible needle at doses of 10-12 units / kg upto a maximum of 200 units. The injection is done at 20-30 sites with 0.5 ml being deposited in each site. The trigone is spared. Excellent results have been reported in the following areas: · Increase in volume of urine held at 20 cms bladder pressure (pressure
specific volume) The results last for six to nine months. In an excellent review article on the use of botulinum toxin; Smith
and Chancellor have added valuable insights in the use of this agent.[15] They
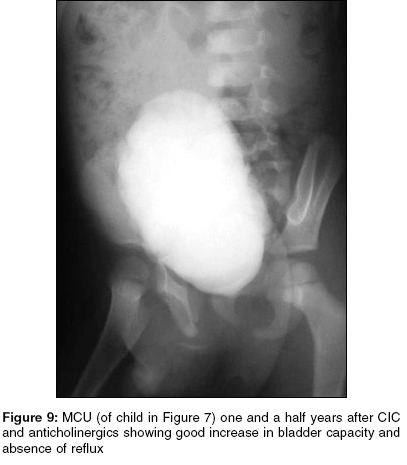
have emphasized the following: The hope is that Botox A may reduce or abolish need for augmentation. However long term results, complications and refractoriness to repeated use of this novel therapy are not known at present (especially in children).[14] In our country, the high cost of Botox A may prevent its widespread use. Non-neurogenic neurogenic bladder or the Hinman Allen Syndrome This represents the end stage of uncorrected dysfunctional voiding. In this condition the changes in the bladder and kidneys are indistinguishable from neurogenic bladder disease. However, in these children, MRI does not show any spinal cord abnormality. Management is identical to neurogenic bladder disease due to spinal anomalies [Figure - 7],[Figure - 8],[Figure - 9],[Figure - 10].[16]Conclusions 40% of children with urinary infections have voiding disturbances and half of them suffer from vesico-ureteric reflux.[3] There is a close relationship between constipation and bladder dysfunction. The elimination of constipation, prompt treatment of urinary infection and behavioral modification will serve to prevent upper tract changes in the long term in these children. Botulinum toxin A is promising to be an effective therapy for those with neurogenic bladder disease refractory to conventional medication. References
Copyright 2005 - Journal of Indian Association of Pediatric Surgeons The following images related to this document are available:Photo images[ip05055f3.jpg] [ip05055f2.jpg] [ip05055f7.jpg] [ip05055f9.jpg] [ip05055f5.jpg] [ip05055f1.jpg] [ip05055f10.jpg] [ip05055f8.jpg] [ip05055f4.jpg] [ip05055f6.jpg] |
| |||||||||

![[Figure - 1]](/showimage?ip/photo/ip05055f1.jpg){kind=link}
![[Figure - 2]](/showimage?ip/photo/ip05055f2.jpg){kind=link}
![[Figure - 3]](/showimage?ip/photo/ip05055f3.jpg){kind=link}
![[Figure - 4]](/showimage?ip/photo/ip05055f4.jpg){kind=link}
{kind=link}
![[Figure - 6]](/showimage?ip/photo/ip05055f6.jpg){kind=link}
![[Figure - 7]](/showimage?ip/photo/ip05055f7.jpg){kind=link}
![[Figure - 8]](/showimage?ip/photo/ip05055f8.jpg){kind=link}
{kind=link}
![[Figure - 10]](/showimage?ip/photo/ip05055f10.jpg){kind=link}