 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
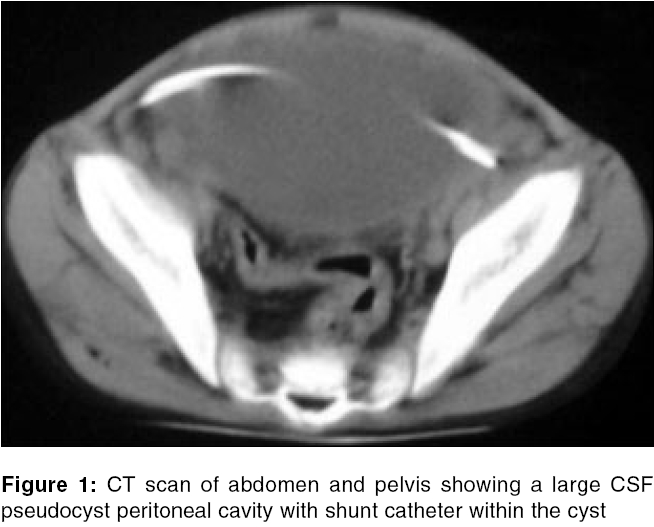
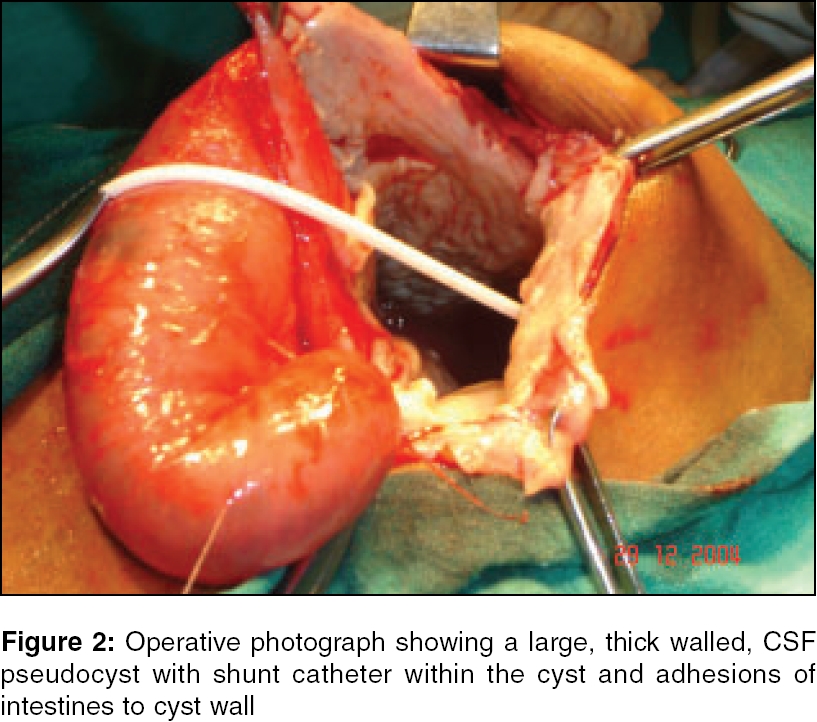
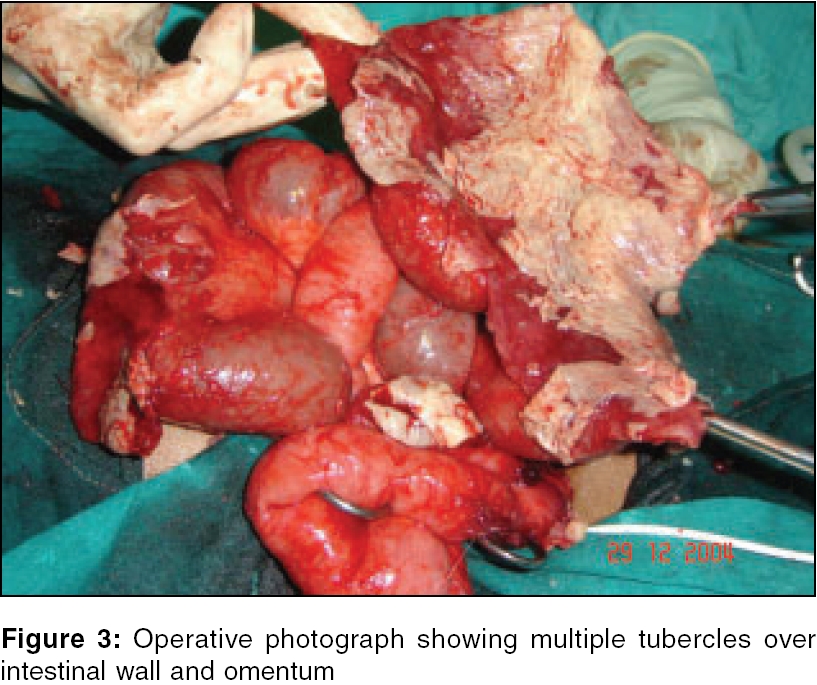
Journal of Indian Association of Pediatric Surgeons, Vol. 11, No. 1, January-March, 2006, pp. 41-43 Case Report C S F pseudocysts peritoneal cavity following V P shunt surgery: Report of three cases in children and review of literature Ghritlaharey RajendraK, Budhwani KS, Shrivastava DK, Jain AJ, Gupta G, Kushwaha AS Department of Paediatric Surgery, Gandhi Medical College and Associated Kamla Nehru and Hamidia Hospitals, Bhopal - 462 001, Madhya PradeshCorrespondence Address:Rajendra K Ghritlaharey, Department of Paediatric Surgery, Gandhi Medical College and Associated Kamla Nehru and Hamidia Hospitals, Bhopal-462 001, Madhya Pradesh, India. E-mail: drrajendrak1@rediffmail.com Code Number: ip06010 Abstract Abdominal cerebrospinal fluid (CSF) pseudocyst is an uncommon complication following ventriculo-peritoneal (VP) shunt. The following report's our experience with three cases of CSF pseudocyst in children. VP shunt was done earlier for communicating hydrocephalus following tubercular meningitis (TBM) in all cases. Clinical presentation was with progressive abdominal distension and features of intestinal obstruction. Clinically we were able to diagnose all cases as CSF pseudocyst peritoneal cavity. Ultrasound examination confirmed the clinical findings in all. CT scan of abdomen and pelvis showed a large unilocular CSF pseudocyst with shunt catheter within it on one patient (case 3). Ultrasound guided aspiration of cyst was done in case 1 alone, but failed to resolve the symptoms. All patients needed formal exploration. Near total cyst excision, adhesiolysis and relocation of peritoneal end of VP shunt catheter in right supra hepatic space was done in all. Two patients who developed shunt tract infection needed shunt removal. The follow up period is 6-8 months.Keywords: CSF pseudocyst peritoneal cavity, V P shunt complication The use of peritoneal cavity for CSF absorption in VP shunting was introduced in 1905, since than VP shunting are among the most frequently performed operations in the management of hydrocephalus. Abdominal complications are reported to occur in 5-47% cases following VP shunt operations.[1] Abdominal CSF pseudocyst is an uncommon but well described complication and reported to occur in < 1% to 4.5% of VP shunt surgery.[2],[5] In 1954, Harsh first described a periumbilical pseudocyst, since than 130 cases of CSF pseudocyst in children have been reported in literature, to which few more cases have been added.[4],[6],[7],[8] Herein we are reporting our experience with 3 cases of CSF pseudocyst peritoneal cavity following VP shunt operation in children. Case Report Case 1 Case 2 Case 3 Discussion Abdominal CSF pseudocyst is an uncommon albeit well-described complication of V P shunt malfunction in children.[2] The exact cause of abdominal CSF pseudocyst formation is still debated. Predisposing factors for CSF pseudocyst formation are; low grade shunt infection, chronic inflammation, multiple shunt revisions, increased CSF protein content, peritoneal adhesions, mal-absorption of CSF secondary to sub clinical peritonitis, silicon allergy, etc.[3],[4] In our series all patients had undergone VP shunt operation for hydrocephalus following TBM. Formation of CSF pseudocyst in our cases was probably due to sub clinical infection . Abdominal CSF pseudocyst may present with features of shunt obstruction, progressive abdominal distension, features of intestinal obstruction, with or without features of raised intracranial tension. The differential diagnosis includes cysts of the mesentery and omentum, abdominal abscesses, ascites, etc.[4] All patients we are reporting here had also presented with abdominal distension and features of intestinal obstruction. Diagnosis of CSF pseudocyst can be confirmed by ultrasound examination of abdomen and pelvis. A small amount of peritoneal fluid can be found with a normally functioning VP shunt. Ultrasonographic evidence of a large localized, or loculated collection of peritoneal CSF is abnormal and suggests CSF pseudocyst.[5] Clinically we were able to diagnose CSF pseudocyst and was confirmed on ultrasound examination of abdomen in all cases. CT scan was done in one patient (case 3), which does not provided any significant additional information. So we also feel Ultrasonography remains an excellent imaging modality for CSF pseudocyst of the abdomen. Traditional staged treatment consists of exploratory laparotomy, removal of shunt / shunt externalization, with or without cyst excision and placement of shunt catheter in different quadrant or conversion of VP shunt to VA shunt. Gaskill et al found that the cyst reabsorbed spontaneously without excision or aspiration once the CSF was diverted. The peritoneal cavity could then be used for re-shunting once the cyst had reabsorbed.[5] In 1995, Kim et al first described the laparoscopic management of a CSF pseudocyst, which involved excision of a portion of the cyst and repositioning the catheter within the peritoneal cavity. Thus a conventional laparotomy along with its various associated postoperative complications is avoided without compromising the quality of surgery.[5] Another way of treating CSF pseudocyst peritoneal cavity is simply conversion of VP shunt to ventriculo - pleural shunt or most frequently to VA shunt.[5],[6],[7] Recently therapeutic ultrasound guided aspiration of CSF pseudocyst in children and adolescents have been advocated in selected patients . In 2004 Coley et al, described this technique and they are of opinion that this is an effective technique, allowing exclusion or confirmation of infection and providing relief of abdominal symptoms in patients with sterile collections, thus staged surgical revision with shunt externalisation can be avoided.[8] We aspirated the cyst twice in case 1, who failed to respond and cyst refilled again within short period of time. Management of CSF pseudocyst must be individualised. We feel cyto-biochemical examination and culture of aspirated fluid must be done if clinical condition of patient permits, so that infection can be ruled out. As we failed to do so and decided on operation table to reposition the shunt in all 3 cases, two of them developed shunt track infection and needed its removal. Once we know the nature of CSF preoperatively, we may opt for repositioning of shunt or shunt exteriorisation rather than deciding on operation table. References
Copyright 2006 - Journal of Indian Association of Pediatric Surgeons The following images related to this document are available:Photo images[ip06010f3.jpg] [ip06010f2.jpg] [ip06010f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}