 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
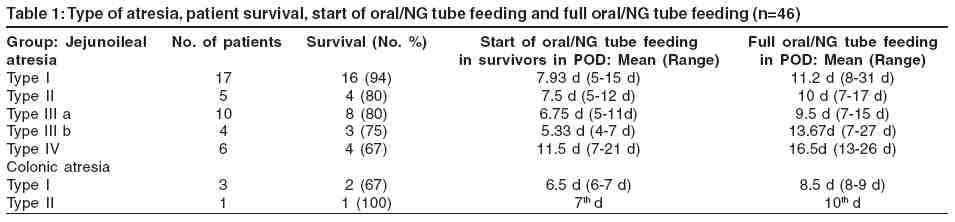
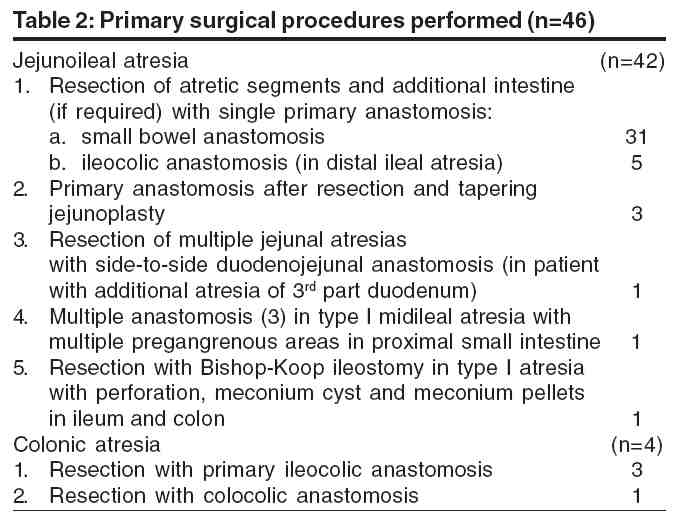
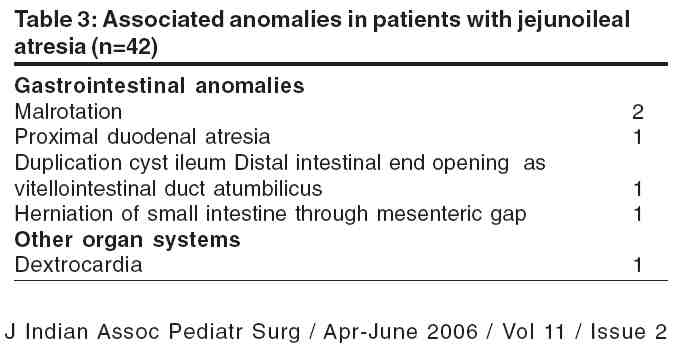
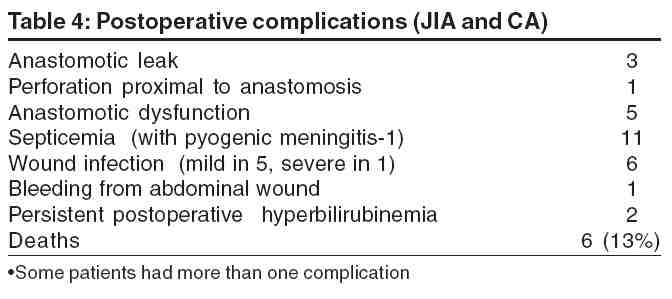
Journal of Indian Association of Pediatric Surgeons, Vol. 11, No. 2, April-June, 2006, pp. 79-84 Original Article Treatment strategies in the management of jejunoileal and colonic atresia Chadha Rajiv, Sharma Akshay, Roychoudhury S, Bagga Deepak Department of Pediatric Surgery, Lady Hardinge Medical College and Kalawati Saran Children's Hospital, New Delhi Code Number: ip06019 Abstract BACKGROUND/PURPOSE: The purpose of this prospective study was to review the operative findings, treatment strategies, as well as the results of management of 46 consecutive cases of jejunoileal and colonic atresia, managed over a 2-year period.MATERIALS AND METHODS: There were 42 patients with jejunoileal atresia (JIA) and 4 with colonic atresia (CA). The 4 group types were: type I-membranous (n=20), type II- blind ends separated by a fibrous cord (n=6), type IIIa- blind ends with a V-shaped mesenteric defect (n=10), type IIIb- apple-peel atresia (n=4) and type IV- multiple atresias (n=6). Primary surgery for JIA consisted of resection with a single anastomosis (n=37), anastomosis after tapering jejunoplasty (n=3), multiple anastomosis (n=1) and a Bishop-Koop ileostomy (n=1). For CA, resection with primary anastomosis was performed. A single end-to-oblique anastomosis after adequate resection of dilated proximal bowel, was the preferred surgical procedure. In the absence of facilities for administering TPN, early oral/nasogastric (NG) tube feeding was encouraged. In patients with anastomotic dysfunction, conservative treatment of the obstruction followed after its resolution by gradually increased NG feeds, was the preferred treatment protocol. RESULTS: Late presentation or diagnosis with hypovolemia, electrolyte imbalance, unconjugated hyperbilirubinemia (n=25) and sepsis (n=6), were significant preoperative findings. After resection and anastomosis, significant shortening of bowel length was seen in 16 patients (34.7%). Postoperative complications included an anastomotic leak (n=3), a perforation proximal to the anastomosis in 1 and anastomotic dysfunction in 5 patients. Full oral or NG tube feeding was possible only by the 13th to 31st postoperative day (POD), after the primary surgery in patients with anastomotic dysfunction and those undergoing reoperation. Overall, 38 patients survived (82.6%). Mortality was highest in patients with type IIIb or type IV JIA. CONCLUSIONS: Despite lack of ideal facilities for neonatal intensive care and administration of TPN, good results were achieved in the management of JIA and CA by following these principles: (1) adequate preoperative resuscitation, (2) meticulous surgical technique and a standardized surgical protocol, (3) early recognition of postoperative complications and their management by a uniform protocol and (4) wherever possible, early institution of oral or NG feeds, preferably by breast milk. Keywords: Jejunoileal atresia, colonic atresia, total parenteral nutrition In 1951, Evans[1] reported a survival rate of 9.3% in patients with gastrointestinal atresia. In the subsequent 2 decades, reported survival rates ranged from 51%[2] to 65%.[3] However, over the last 2 decades or more, most reports from developed countries describe survival rates approximating or greater than 90%, for patients with jejunoileal atresia (JIA). [4],[5],[6],[7] Prognosis in cases of colonic atresia (CA) is also usually excellent. This reduction in mortality has largely been due to better understanding of etiologic factors, recognition that the dilated bowel proximal to the atretic segment was dysfunctional leading to modifications in surgical procedures, improved anastomotic technique and suture material, improvement in various aspects of neonatal care and anesthesia, as well as the development of total parenteral nutrition (TPN).[7],[8] However, in developing countries like ours, the results are still not satisfactory. [9],[10],[11] Reported mortality rates following surgery for JIA, range from 41%[11] to 68%.[10] This report describes a series of 46 patients with JIA and CA, managed over a 2-year period, in a specialized children′s hospital in New Delhi, India. The modifications in management strategies, necessitated both by the clinical status of the patients, as well as the availability of investigative and management facilities, are discussed in detail. Materials And Methods During the 2-year period from March 1999 to 2001, a detailed case-record of 46 consecutive patients treated for JIA and CA, was maintained. There were 42 patients of JIA and 4 patients of CA. The gestational age was between 29 to 42 weeks (mean=38 weeks). The weight at presentation was between 1.38 to 3.34 kg (mean= 2.21 kg), while age at presentation ranged from 0 to 20 days (mean=5.62 days). 15 patients (33%) were more than one week old at presentation, having been managed at primary/secondary health centers prior to referral to our institution. The 46 patients were classified into the four group types described by Grosfeld et al : [12] I, (n=20, 43.4%); II, (n=6, 13%); IIIa, (n=10, 21.7%); IIIb, (n=4, 8.7%); IV, (n=6, 13%). The grouping of the patients is shown in [Table - 1]. The management strategy for the patients is outlined as follows. After initial evaluation, a nasogastric (NG) tube (6 to 8 Fr.) was placed for gastric decompression. In the usual patient, a bolus of 20 ml/kg body weight of lactated Ringer′s solution was administered over a 30 minute period, to correct the fluid and electrolyte losses. Depending upon the clinical and biochemical assessment of hypovolemia and electrolyte imbalance, additional lactated Ringer′s solution or half-strength Ringer′s lactate in 10% dextrose was administered, to correct fluid losses and maintain an adequate urine flow. A 5% dextrose in 0.20% normal saline solution was employed for maintainence fluid requirements. The presumptive diagnosis and decision regarding the need for surgery was based on clinical findings and examination of plain abdominal radiographs, in all patients. As a routine, preoperative antibiotics were administered in the form of a cephalosporin, gentamicin/amikacin and metronidazole. The time-interval between the presentation and the surgery, varied from 6 hours to 2 days. In several patients, this delay was necessitated by the need for prolonged preoperative resuscitation. In some cases of uncomplicated JIA or CA, the delay was due to temporary lack of availability of a well-equipped, dedicated pediatric surgery operation room (OR). The operative procedures performed during primary surgery on the 46 patients, are shown in [Table - 2]. At laparotomy, the bowel length was measured and the distal bowel injected with saline, to ensure patency down to the level of the rectum. In the usual case of a single JIA, 5 to 25 cm of proximal bowel and 2 to 10 cm of distal bowel was resected. The general principle was to resect proximal intestine till 1 to 2 inches (2.5 to 5 cm) distal to the ligament of Treitz in proximal jejunal atresia and a diameter of 1.0 to 1.5 cm in ileal atresia.[8] Division of vascularized, often dense adhesions, correction of malrotation and/or volvulus, closure of intestinal perforation(s) and resection of bowel with compromised vascularity, was performed where required. In general, enterostomies were avoided and a primary anastomosis was performed wherever possible. In order to avoid an inordinately long operating time wherever possible, if total usable jejunoileal length was adequate (>75 cm), even in cases with multiple atresias, multiple anastomoses were avoided and a single end-to-oblique anastomosis performed. The anastomotic technique consisted of interrupted, inverting, horizontal mattress sutures (Connell sutures) of 5-0 Vicryl (polyglactin) or 5-0 PDS, placed in both anterior and posterior layers, utmost care being taken to avoid narrowing at the mesenteric and antemesenteric corners. Reinforcing Lembert (seromuscular) sutures were placed where required and wherever feasible, generally in cases of proximal jejunal or distal ileal atresia, the anastomotic line was reinforced with omentum. In the 4 cases of CA, the atresia was at the level of the ascending colon in 2 patients and at the level of the hepatic flexure in the other 2 patients. Postoperatively, NG tube decompression of the stomach, intravenous fluids and antibiotics were continued. If stools were not passed by the 4th to 6th postoperative day (POD), daily administration of a low-volume glycerine-saline enema (2 ml glycerine with 3 ml saline) for one or two days, was found to be useful. After passage of stools and when the NG aspirate was clear and less than 30 ml/day, low volume feeding with milk, preferably by breast feeding or by expressed breast milk (EBM) administered through a narrow gauge (5 to 6 Fr) NG tube was started and gradually increased till total oral or enteral nutrition could be instituted. In some patients, due to anastomotic dysfunction or other factors, early oral or NG tube feedings could not be instituted, or else had to be discontinued. In the absence of availability and facilities for administering TPN, nutrition was maintained in these patients by maintainence fluid of 0.20 % saline in 10% dextrose solution at 150 ml/kg/day, electrolyte supplementation, plasma transfusion (10 ml/kg/day daily or on alternate days) and transfusion of multivitamin and trace elements solutions. After restoration of enteral function, often after a period of several days, low-volume (usually 3 to 5 ml initially every 3 hours) enteral NG tube feeding of EBM was started, with precautionary aspiration of the stomach, before every feed. EBM feeds were increased gradually over 5 to 7 days or even longer, till total enteral nutrition (TEN) was achieved. In some small, premature infants and also in some emaciated, malnourished babies, even after TEN was achieved, NG tube feeding was continued for some days, until it was felt that the child was strong enough to suckle at the mother′s breast. Thereafter, oral feeding was gradually increased and simultaneously NG tube feeding volumes gradually decreased till full oral feeding was established, usually over a period of 2 to 5 days. Results Apart from the usual clinical findings, significant icterus due to unconjugated hyperbilirubinemia was noted in 25 patients (54%), including 2 patients with CA. At admission, 16 patients (35%) had moderate to severe hypovolemia and dehydration with concomitant electrolyte imbalance. Bronchopneumonia was present in 2 patients, while clinical and bacteriological evidence of septicemia was present in 6 patients (13%). Prior to transfer to our surgical unit, 4 patients were suspected initially to have neonatal septicemia and/or hyberbilirubinemia with septic ileus and were managed in the pediatric wards of our hospital for 5 to 9 days. The associated anomalies detected in the 42 patients of JIA, are shown in [Table - 3]. In addition, evidence of intrauterine intestinal perforation with multiple adhesions and localized meconium peritonitis, often with matting of small intestinal loops, was noted in 12 patients (26%). In one patient, there was dense intraperitoneal calcification, while 4 patients (9%) had a meconium cyst. Volvulus of the proximal small intestine without malrotation was noted in 2 patients, one with intestinal gangrene. An additional 4 patients had gangrene or compromised vascularity of the small bowel; in one of these, the ileum, proximal to the atretic segment, was completely autolysed with severe fecal peritonitis. In 3 patients, although there were no other features suggestive of meconium ileus, the small intestinal segment distal to the atresia was packed with discrete mucoid pellets, till the ileocecal valve. In the 4 patients of CA, no other abnormality was detected. After corrective surgery in the 36 patients with types I to III JIA, small intestinal length was adequate i.e.,> 75 cm[13] in 23 patients (64%). Significant shortening of bowel was seen in 13 patients (36%), including 3 out of the 4 patients with type IIIb atresia, the residual small bowel length ranging from 30 to 75 cms. These included 10 patients with an intact ileocecal valve and 3 with an ileocolic anastomosis. In the 6 patients with type IV JIA, normal residual small bowel length was present in 3 patients, while 3 patients, all with an intact ileocecal valve, had small bowel length of 22 cm, 35 cm and 60 cm, respectively. The residual small bowel length in all patients with CA, was adequate. The postoperative complications are shown in [Table - 4]. Three of the 5 patients with anastomotic dysfunction were successfully managed conservatively by the management protocol outlined earlier. Low-volume NG tube feeds of EBM were begun from the 13th to 18th POD and TEN by the NG route was possible by the 16th to 24th POD. In one patient, during the phase of anastomotic dysfunction, the parents were unwilling to wait and took the child home on the 10th POD. Reoperation, always by a senior, experienced pediatric surgeon, was necessary in 5 patients due to an anastomotic leak (3), a perforation proximal to the anastomosis (1) and for prolonged anastomotic dysfunction (1). In patients with an anastomotic leak, dismantling of the anastomosis, excision of 2 to 3 cm bowel on either side and reanastomosis was performed in 2 patients, while simple reinforcement of the anastomosis was performed in one patient. Prolonged anastomotic dysfunction in a patient with type IV jejunal atresia and a proximal duodenal atresia, necessitated refashioning of a 2.5 cm wide duodenojejunal anastomosis. All patients who underwent reoperation were successfully managed postoperatively by the protocol detailed above, the time-interval (from the first surgery) before starting NG tube feeding varying from 11 to 24 days, TEN being achieved by the 13th to 31st day. Sepsis and septicemia was managed by appropriate changes in antibiotic therapy. One child had Escherischia Coli septicemia and another had Klebsiella sepsis. Overwhelming Candida sepsis occurred in one patient of type I CA. There were 6 deaths in this series. Death occurred on the 1st to 9th postoperative day. The causes of death included overwhelming sepsis in 5 patients, one with additional pyogenic meningitis. Other causes or contributory factors included severe bronchopneumonia (1), preexisting fecal peritonitis (3), extensive bowel gangrene with autolysis of bowel (1), hyperbilirubinemia (5), severe hypovolemia with electrolyte imbalance (2) and extreme malnourishment (2). Prematurity was also a factor; 3 deaths were of premature babies with a weight ranging from 1.38 to 1.67 kg. In one patient of type IV jejunal atresia with numerous small atretic segments, 22 cm of small bowel remained after resection and anastomosis. The parents were advised against continuing medical therapy, as facilities for administering TPN were not available. Overall therefore, 38/46 patients survived, a survival rate of 82.6%. The lowest survival was seen in type IIIb atresia (75%) and type IV atresia (67%). During a follow-up period of 4 years, 2 patients were admitted at the age of 3 weeks and 2 months respectively, for treatment of enterocolitis, hyperbilirubinemia,and sepsis. Both patients were managed successfully with antibiotics and supportive therapy. An operated case of type I ileal atresia was admitted at the age of 1 month with adhesive intestinal obstruction, which resolved on conservative therapy. Five other patients, all with short bowel (35-60 cm), were admitted or treated as outpatients, several times, for diarrhea and nutritional deficiencies. After treatment of dehydration, these patients were discharged on vitamin supplementation and advice, regarding nutrition and feeding. Discussion In developing countries, the poor nutritional status of the patients, late presentation or diagnosis, improper or inadequate management at primary and secondary health centers, lack of availability or accessibility to good neonatal intensive care centers and lack of nutritional support, are the primary reasons for the high mortality rates reported in patients with bowel atresias. [9],[10],[11] Management strategies therefore, have to be modified, considering the clinical status of the patients and the deficiencies in investigative and management facilities. A significant feature in this series was the delayed presentation of several patients. The resultant high incidence of preoperative hypovolemia, dehydration, electrolyte imbalance, sepsis, pneumonia and unconjugated hyperbilirubinemia, undoubtedly has an adverse effect on the prognosis.[2],[14] Late referral of patients, initially admitted in overcrowded pediatric medical units in our own institution, is also an adverse prognostic factor. As shown by this study, delay in presentation or management also increases the incidence of secondary gastrointestinal problems such as bowel gangrene, intestinal perforation and intestinal volvulus. In our study, clinical findings and plain abdominal radiographs were found to be sufficient to make a diagnosis and to take a decision regarding the need for surgery. Although it has been stated that if a preoperative contrast enema is not performed, this can result in failure to diagnose an additional colonic or rectal atresia. [15],[16],[17] Careful inspection of the bowel during surgery and milking of saline in the distal segment right down to the rectum, obviates the necessity of performing routine preoperative contrast studies. The value of preoperative resuscitation and adequate correction of hypovolemia and third-space losses, especially in cases where presentation has been delayed for several days, cannot be overemphasized. The principles enunciated by Filston[18] regarding perioperative fluid therapy in newborns and infants undergoing major gastrointestinal surgery, are invaluable in this regard. From the point of view of the ultimate outcome, perhaps the most important factor is that surgery should be performed either by, or under the supervision of an experienced pediatric surgeon and a uniform surgical protocol should be followed. We believe that wherever residual small bowel length will be adequate i.e., more than around 75 cms,[13] liberal resection of proximal dilated bowel with a single end-to-oblique anastomosis, every attempt being made to preserve the ileocecal valve, is the most desirable option and is usually safe and effective. In recent reports, multiple anastomoses (upto 7 in number) have been advocated by several authors in order to increase the available intestinal length in type IV atresia. [19],[20],[21] However, multiple anastomoses do lead to increased morbidity[2],[22] and in addition, an inordinate increase in operating time is often not conducive to a favorable outcome in our institutional setup. Fortunately, multiple atresias are usually localized,[22] so that resection with a single anastomosis is very often an appropriate surgical option. It has been suggested that in JIA, resection of the dilated proximal bowel should be minimized, as central venous TPN can tide over the period of dysmotility and impaired anastomotic function.[20] However, preservation of as much bowel length as possible at the risk of creating a poorly functioning anastomosis, has little merit and can produce significant morbidity and mortality.[3],[17] This is especially important if facilities for administration of TPN are lacking, as at our center. We also believe that after resection, creation of a wide end-to-oblique anastomosis by slitting open the distal bowel until its diameter easily equals that of the proximal bowel, reduces the risk of anastomotic dysfunction. In this series, we preferred to avoid stomas whenever possible, as the consequent fluid and electrolyte losses may be severe and very difficult to manage, both in our institutional setup, as well as by the parents at home. Creation of stomas in patients operated for bowel atresias also increases chances of sepsis, morbidity and mortality.[1],[2],[17] Even in the presence of fecal peritonitis or bowel gangrene, a primary anastomosis is usually possible and gives good results. Early recognition of anastomotic leak or peritonitis is essential. Clinical findings are usually adequate for this purpose.[17],[23] Reoperation should be performed as early as is possible and during the second surgery, creation of a stoma can still be avoided, as reanastomosis or refashioning of the original anastomosis is usually a safe surgical option. Recent large series describe the use of short-term/long-term TPN in as many as 23 to 73% of patients of JIA.[7],[8],[20] Use of TPN is especially useful in patients with type IIIb atresia, type IV atresia, or in cases with short-bowel syndrome.[17] In the absence of availability of TPN, early restoration of oral or some form of enteral feeding becomes essential. However, due to the factors detailed earlier, in some instances, our patients were well more than one month old by the time full oral feeding or TEN by NG feeding was established. Thus, although the management protocol described here for patients with significant delay in initiation of oral/enteral feedings was successful in the ultimate outcome, short-term morbidity was severe, as the babies were maintained in a catabolic state with protein-calorie-lipid-malnutrition for prolonged periods of time. CA is a rare form of bowel atresia[15] and comprised of 8.7% of the total patients in our series. Prognosis was good, 3 of the 4 patients surviving resection and primary anastomosis for right-sided atresias. Despite the adverse prognostic factors as detailed earlier, the overall survival in our series (82.6%) is comparable to the survival figures of 86 to 96.7%, described in recent large series of JIA reported in the literature. [6],[7],[8],[21] Certain long-term problems however, deserve special consideration. Significant shortening of residual small bowel length was seen in 16 patients (38%) of JIA. Ideally, these patients would be candidates for long-term institutional/home TPN, or else, the prolonged use of elemental or other special diets, administration of growth hormone and glutamine and/or other growth factors.[8],[17] None of these alternatives are available at our center. This series also does not take into account, late morbidity and mortality. Grosfeld[8] reported 16 late deaths from 3 to 8 years after initial treatment, in his series of 136 patients. In summary, despite lack of availability of TPN and other intensive-care facilities, the results achieved by us can be said to be due to several factors: (1) the incidence of major associated anomalies involving other organ systems is low in JIA and CA and thus, absence of excellent neonatal intensive care facilities was not a major handicap, (2) adequate preoperative correction of hypovolemia, third-space losses and electrolyte imbalance, with the use of prophylactic antibiotics in all cases, (3) surgery in a dedicated pediatric surgery, OR with an experienced pediatric surgeon and pediatric anesthetist in attendance, (4) meticulous surgical technique and a standard surgical protocol, (5) early recognition of postoperative anastomotic leak or peritonitis with prompt reoperation, (6) wherever possible, early institution of oral or NG tube feeding with breast milk and (7) management of anastomotic dysfunction by a uniform protocol, as detailed earlier. It is possible to achieve further improvement in both short-term and long-term results if, for example, facilities for administration of TPN and/or elemental diets are available. Although the deaths in this series occurred 1 to 9 days after primary surgery and thus malnutrition was not the primary responsible factor, undoubtedly malnutrition predisposes to intercurrent infections, septicemia, hemorrhagic disorders and multi-organ failure. Although not employed by us, a transanastomotic tube for feeding may help maintain adequate enteral nutrition in cases of high atresia with marked dilatation of the proximal bowel and thus avoid the consequences of anastomotic dysfunction.[17] References
Copyright 2006 - Journal of Indian Association of Pediatric Surgeons The following images related to this document are available:Photo images[ip06019t1.jpg] [ip06019t3.jpg] [ip06019t4.jpg] [ip06019t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}