|
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
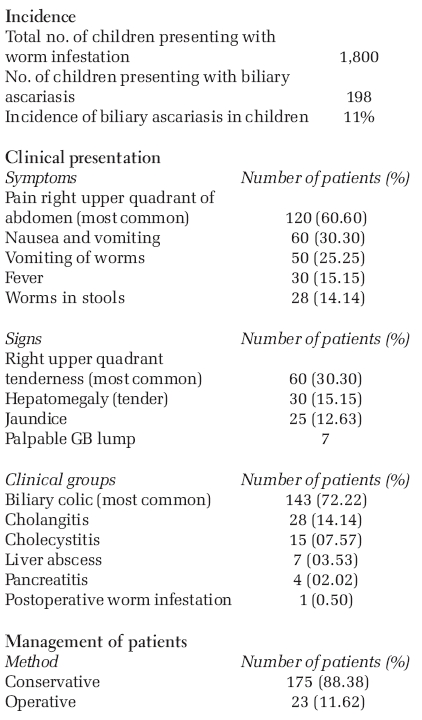
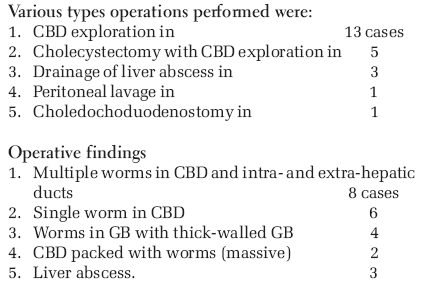
Journal of Indian Association of Pediatric Surgeons, Vol. 11, No. 3, July-September, 2006, pp. 129-132 Original Article Our experience of biliary ascariasis in children Wani MY, Chechak BashirA, Reshi Farooq, Pandita Sanjay, Rather MuddasarH, Sheikh TariqA, Ganie Ishfaq Department of Surgery, GMC, Srinagar, Jammu and Kashmir Code Number: ip06032 Abstract Ascariasis is highly endemic in Kashmir valley as temperate climate and wet soil provide excellent conditions for its development. We studied 198 cases (11%) of biliary ascariasis out of 1,800 patients of worm infestation from December 2001 to December 2004 in the age group of 4-15 years. In our study, we found biliary ascariasis to be more common in female children, and most common clinical presentation was biliary colic in 143 patients, cholangitis in 28, cholecystitis in 15, liver abscess 7, pancreatitis 4 and postoperative worm infestation in 1 patient. Ultrasonography of abdomen was the diagnostic tool of choice with hundred percent results. Most of the patients were managed conservatively. ERCP was not done in children because of need of general anesthesia and difficulty in performing the procedure. Surgical intervention was required in 23 patients (cholecystectomy with CBD exploration in 5, choledochotomy alone in 13, drainage of liver abscess in 3, choledochoduodenostomy in 1 and peritoneal lavage in 1).Keywords: Biliary ascariasis, biliary colic, ultrasonography History of ascariasis is known to stretch back many centuries. Ascaris lumbricoides, a nematode, is the causative agent of ascariasis . It is the most common helminthic infection in the world, with an estimated worldwide prevalence of infection in more than 1 billion people, with majority in the developing countries of Asia and Latin America. In our Kashmir valley, ascariasis is endemic, especially in the pediatric age group. It affects mainly children from low socio-economic group, whose standard of living and personal hygiene are poor. Poverty, unhygienic conditions, poor sanitation and unsafe drinking water supply contribute to the spread of infection. The wet soil of Kashmir and temperate climate are excellent conditions for the development of larval stage of worms. The adult roundworm normally lives in the small intestine, but due to 'wanderlust' nature of the worms and their tendency to explore orifices, ducts and cavities, the worms often invade the bile or pancreatic ducts. Three phases of ascariasis may be present - namely, the pulmonary, intestinal and the complications stage. Although generally asymptomatic, heavy infestation may cause serious complications like intestinal obstruction, biliary colic, cholecystitis, cholangitis, liver abscess, peritonitis, pancreatitis and loeffler's pneumonitis. Most of the patients of biliary ascariasis respond to conservative treatment, but some patients need surgical intervention. Aims and objectives The purpose of this study was to determine the incidence of biliary ascariasis in the pediatric age group of Kashmir and to assess various options for management of biliary ascariasis in children, with emphasis on surgical options and its indications.Materials and methods This prospective study was conducted at Government Medical College Hospital (SMHS), Srinagar, in the Pediatric Surgery Division of Department of Surgery, from December 2001 to December 2004. A total number of 198 (males 49 and females 149) children with biliary ascariasis were studied, aged between 4 and 15 years, belonging to various regions of Kashmir valley. In our study, detailed clinical assessment was done in every case. History of passage of worms in stool or vomiting and recurrent abdominal pain, with or without jaundice, was taken in each case. Complete blood cell counts, liver function test, serum amylase, X-ray chest, X-ray abdomen and ultrasound abdomen were done in all patients at the time of admission and repeated when required. The white blood cell count was moderately raised with eosinophilia; the liver function tests were normal in uncomplicated cases. LFT was markedly deranged in 20 patients and moderately in 35 patients; serum amylase was raised in 4 patients. The mainstay of diagnosis was ultrasound abdomen with focus on hepatobiliary system. All our patients were initially managed conservatively with intravenous fluids, IV antibiotics and IV antispasmodics. All patients were de-wormed with a single dose of 400 mg of albendazole. Spasmolytics were also given to relax sphincter of oddi to release the worms. Surgical intervention was done where conservative treatment failed. Patients were followed for 6 months with serial USG for any recurrence. All patients were de-wormed with a single dose albendazole 400 mg at intervals ranging from 3 to 6 months. Results
About 90% of patients responded to conservative therapy with nothing per oral, Ryles tube suction, intravenous fluids, antibiotics, antispasmodics and antihelmenthics. Most of the patients responded to this treatment in 3-5 days. In some patients, the above treatment had to be continued for 1 week or more. Patients were monitored by serial ultrasound to know the status of worms in biliary tree. Twenty-three patients were operated, and indications for surgery were- cholecystitis with worms in GB, cholangitis not responding to conservative treatment, progressively increasing jaundice, pyrogenic liver abscess, persistent upper abdominal pain not responding to conservative treatment and massive hepatobiliary ascariasis.
T tube was put in all those patients where CBD was explored. In the postoperative period, T tube was clamped on 5th postoperative day onwards and cholangiogram was performed on 10th to 12th day. T tube was removed by the end of the 2nd week if there was no obstruction in the CBD. One patient had postoperative recurrence documented by USG and postoperative cholangiogram, which was successfully managed by normal saline washes via T tube and oral antihelmenthic drugs. Only one patient, who had suppurative cholangitis with multiple liver abscesses with septicemia, died in postoperative period. Patients were followed up for 6 months with serial USG. Regular de-worming was done in all patients with single dose of albendazole (400 mg). Recurrence of biliary ascariasis was seen in nine non-operated patients and in one postoperative patient. Discussion During the life cycle of ascaris lumbricoides, the larvae of this worm are hatched in the duodenum. From here, they enter the portal vein and then lungs and back to gut.[1] After completion of life cycle, some of the adult worms in duodenum enter into the CBD and/or pancreatic duct. Ascariasis worms have 'wanderlust' and tend to explore ducts and cavities.[2] Incidence of biliary ascariasis is very high in endemic areas, particularly when there is heavy infestation of duodenum with worms. In our study, the incidence of biliary ascariasis was 11%, i.e., 198 patients out of 1,800 intestinal worm infestations. Usually, only one or two worms enter the CBD-producing features of acute uncomplicated biliary ascariasis.[1] If worms remain in bile ducts, acute and chronic complications can occur, like cholangitis, strictures, calculi, cholecystitis and pancreatitis.[3] Some worms may travel up and colonize in liver parenchyma forming liver abscesses.[4] Liver abscesses are usually small and multiple but are occasionally large and can rupture.[3] Massive hepatobiliary ascariasis is uncommon. In our series, only 2 patients had massive hepatobiliary ascariasis. Lloyd DA recorded 9 patients with massive hepatobiliary ascariasis.[4] The clinical features of acute biliary ascariasis are well established.[5],[3] Pyrexia with right upper quadrant pain and tender hepatomegaly is suggestive of cholangitis and / or hepatic invasion.[7],[9] Worms cause malnutrition, especially in growing children.[5],[2] The diagnosis of biliary ascariasis usually depends on the demonstration of worms in the biliary tract by different imaging techniques (IV cholangiography, per operative cholangiography, ERCP, USG). USG scanning is a safe, noninvasive, accurate and readily available tool for diagnosing biliary ascariasis and its complications.[6],[4] More than 95% of patients with uncomplicated biliary ascariasis will respond to conservative management, the worms returning spontaneously to intestine.[3],[4] The return of worms is enhanced if the gut is cleared of worms by administering anti-helminthics, but the drugs should be given continuously when the gut is heavily infested with worms, as there is a risk of precipitating intestinal obstruction.[4] Pyrantel pamoate, mebendazole, albendazole and levamisole are effective.[5] Newer drugs like Ivermectol have also shown good results. Single or multiple worms in CBD without invasion to liver respond mostly to conservative therapy.[4] Indications for operative management in our study were similar to that of Lloyd and Louw.[3],[4] We recommend conservative management while investigations are undertaken and a course of anti-helminthic is commenced. If the clinical picture is unrelieved or if the patient has complicated biliary ascariasis, conservative treatment should be abandoned in favor of early operative treatment to avoid complications.[7] The objective at operation is complete clearance of worms from biliary channels and intestine. T tube drainage is recommended. If a large number of worms are found in the intestine, they should be evacuated by enterotomy to prevent postoperative re-infestation, but this is not necessary if patients are given preoperative anti-helminth therapy. Patients require appropriate antibiotic therapy in postoperative period. Anti-helminths are given when bowel function returns. T tube cholangiogram is performed before removing the T tube, to exclude re-infestation of the biliary tree by residual hepatic or intestinal worms. Most patients recover after operation, but fatal septicemia may result when treatment is delayed.[8] The single death in our series was due to suppurative cholangitis with multiple liver abscesses with septicemia. Conclusion Most of the patients of biliary ascariasis respond to conservative treatment. Early surgical intervention is advisable in patients not responding to conservative treatment, to avoid serious complications. USG is an effective tool for diagnosis and monitoring the treatment response. The solution to the problem of biliary ascariasis does not lie in surgical intervention but prevention by means of providing safe drinking water, proper disposal of night soil, good hygiene and de-worming of all children in endemic areas at regular intervals. We suggest that there should be a national program for eradication of worms in endemic areas. References
Copyright 2006 - Journal of Indian Association of Pediatric Surgeons |
| |||||||||