 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
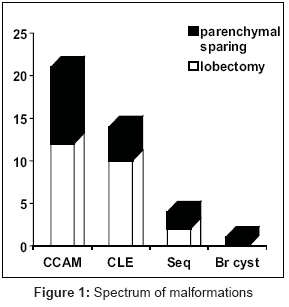
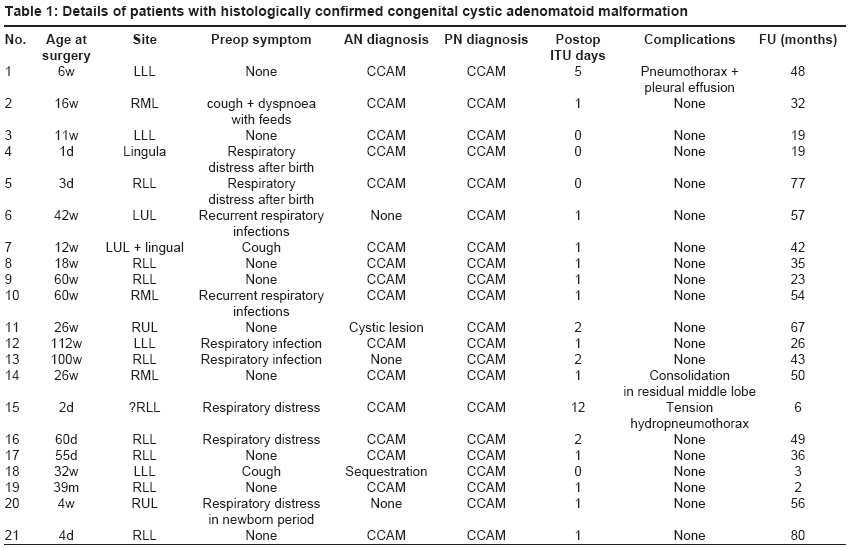
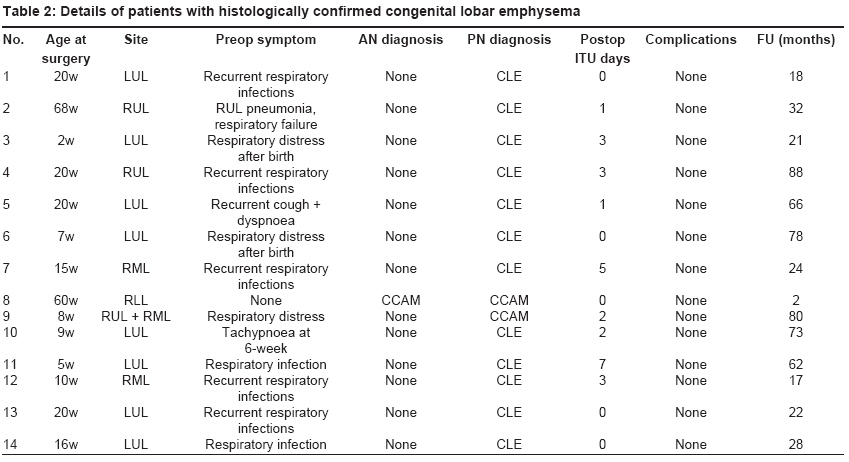
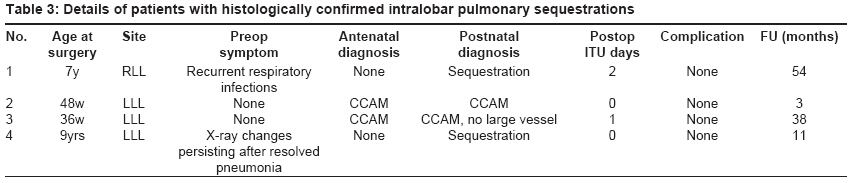
Journal of Indian Association of Pediatric Surgeons, Vol. 13, No. 3, July-September, 2008, pp. 111-114 Original Article Open resections for congenital lung malformations Mullassery Dhanya, Jones MatthewO Department of Pediatric Surgery, Royal Liverpool Children's Hospital, Alder Hey, Liverpool, L12 2AP Code Number: ip08036 Abstract Aim: Pediatric lung resection is a relatively uncommon procedure that is usually performed for congenital lesions. In recent years, thoracoscopic resection has become increasingly popular, particularly for small peripheral lesions. The aim of this study was to review our experience with traditional open lung resection in order to evaluate the existing "gold standard." Keywords: Pediatric lung resections, thoracotomy Introduction Pediatric lung resection is most commonly performed for congenital malformations, which include congenital cystic adenomatoid malformations (CCAMs), congenital lobar emphysema (CLE), sequestrations and bronchogenic cysts. The rate of resection has increased in recent years owing to improvements in antenatal detection, with the result that many asymptomatic lesions are being removed on the basis that they pose a future risk of infection or malignancy. [1] Traditionally, open resection and /or lobectomy has been the procedure of choice; however, a number of surgeons are now advocating the use of minimally invasive techniques on the grounds that this may lead to an improved outcome. [2] The purpose of this study was to review our experience with open resection in order to establish whether there might be a significant scope for improvement.Materials and Methods This was a retrospective review. All patients with congenital lung lesions who had open resection by a single surgeon at our institution between August 1997 and November 2004 were included in the study. Patients undergoing thoracotomy for infective or malignant lesions were excluded. Data were collected from a review of case notes, operative records and patient examination. The data were analyzed using SPSS (SPSS version 12.0.1 for Windows, SPSS Inc., Chicago, IL, USA).Results Forty-one patients (28 M/13 F) with a mean age of 4.7 months were included in the study. The final patient who is not on the list was a 16 year old who presented with a lung abscess. The histology of his lobectomy showed evidence of CCAM. This patient was excluded from the final analysis as this is atypical, and because we do not have definite evidence to suggest that the CCAM was the pathology behind his lung abscess at such a late age. The lung lesions included 21 CCAMs (51.2%), 14 CLEs (34.1%), four sequestrations (9.8%) and one bronchogenic cyst (2.4%). Twenty-one (51.2%) of these lesions were diagnosed antenatally and 28 (70%) were symptomatic. Twenty-six (63%) lesions were removed by lobectomy and 15 (37%) by parenchymal sparing resection of the lesion alone [Figure - 1]. There were no operative or perioperative complications. Blood loss was minimal and no patient required transfusion. Most infants were extubated at the end of the procedure and the mean ITU/HDU stay was 1.7 days (range 0-12 days) .The mean inpatient stay was 5.7 days (range 3-13). These results are skewed by a single infant with a giant CCAM that was causing gross mediastinal shift, hydrops and extreme respiratory difficulties. An initial debulking procedure was performed to help ventilation, followed 3 days later by a definitive resection. Details of the patients in the major diagnostic groups are summarized in [Table - 1] (CCAM), [Table - 2] (CLE) and [Table - 3] (intralobar sequestration). Mean follow-up was for 39 months (range 2-88 months) and there were no complications. No patient had developed any chest deformity, although one child, who had two lobes resected, had a minor degree of chest asymmetry. All the patients were alive and well at the time of the study. Discussion Lung resection is an infrequent procedure in the pediatric population. Although lung resection may be performed for infective or neoplastic lesions, the vast majority of resections are now performed for CCAMs, CLEs and sequestrations. While some of these lesions may present acutely, the majority are asymptomatic [3],[4],[5] and, traditionally, such patients would only ever have presented in the event of serious complications. In recent decades however improvements in antenatal sonography have led to a huge increase in the detection of asymptomatic lesions [1],[6],[7],[8],[9] and the exact role of surgery has become highly controversial. [10],[11] In the absence of comprehensive data, [10] it is difficult to assess the relative risks of operative and nonoperative management. While it is clear that many lesions are completely innocent, [12],[13],[14],[15] it has been suggested that others may pose a significant risk of future infection [10],[16],[17],[18],[19] or even malignancy. [20],[21],[22],[23],[24],[25] At this present time, surgical strategies vary widely from the "very conservative" [6] to the "very aggressive." [1],[3],[4],[26] In our institution, we have adopted a pragmatic practice of removing lesions that are symptomatic, large or air filled. In recent years, video-assisted thoracoscopy (VATS) has become increasingly popular in adult thoracic practice. The first recorded use of VATS in children was by Rodgers [27] in the late 1970s and, more recently, other authors have published series showing it to be a safe and effective technique in experienced hands. [2],[28],[29] By and large, such lung resections have either been nonanatomical resections of small peripheral lesions or complete anatomical lobectomies, [2],[29] a choice of procedure that perhaps reflects the limitations of the technique. A recent small series [30] has reported the use of VATS for lung-sparing resection, and it would appear that such a technique is at least feasible, if not exactly easy. The potential advantages of VATS are considerable, and these include better cosmesis, less discomfort, shorter hospital stay and reduced deformity. [2],[30] However, these need to be balanced against the potential disadvantages, which include greater operative risk, longer operative time, increased operative cost and unnecessary loss of normal lung tissue. [2],[28] In the final analysis, open thoracotomy will always be quicker, cheaper and safer in most surgeons′ hands and the potential advantage of VATS, therefore, rest upon there being a significant incidence of the problems that it claims to avoid. We use as small a skin incision as possible followed by a muscle-sparing approach through the 5 th or the 6 th intercostal space, depending on the location of the lesion (i.e. upper lobe or lower lobe).We routinely use a thoracic epidural for optimal pain management and always leave a chest drain postoperatively. In our series, there were no operative, perioperative or postoperative problems. The vast majority of patients made a prompt recovery and were discharged within 6 days. There has not been a single case of scapular winging or chest deformity and in only one case is there a detectable degree of chest asymmetry. This child is quite interesting in that he had both the right middle and lower lobes resected and it seems likely that his asymmetry reflects the relative absence of underlying lung tissue. With this in mind, it would seem that the best way to avoid deformity might be to do an anatomically exact lung-sparing resection, a technique which has so far proved quite difficult with VATS. We conclude that open resection of congenital lung lesions is a simple, safe and inexpensive technique, which produces excellent results both in the short and medium term. At the present time, we feel that this should remain the "gold standard" against which newer techniques must be judged. References
Copyright 2008 - Journal of Indian Association of Pediatric Surgeons The following images related to this document are available:Photo images[ip08036f1.jpg] [ip08036t2.jpg] [ip08036t3.jpg] [ip08036t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}