 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
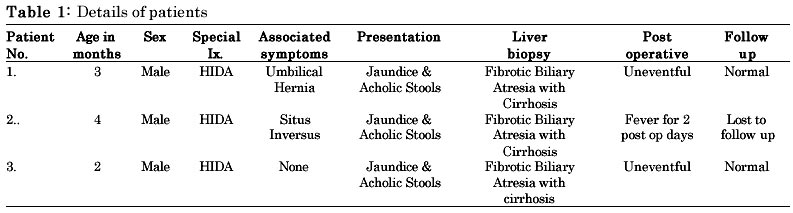
Indian Journal of Surgery, Vol. 64, No. 6, Nov - Dec. 2002, pp. 496-498 Appendix as a Biliary Conduit in Children with Biliary Atresia Amar A. Shah, Anirudh V. Shah Department of Pediatric Surgery, K. M. School of Postgraduate Medicine & Research,
N. H. L. Municipal Medical
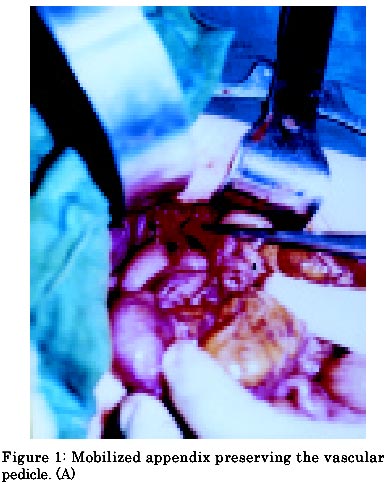
College, V.S. Hospital, Ahmedabad, India Paper received: January 2002 Code Number: is02003 Abstract Biliary conduits are constructed during operations for biliary atresia. A wide variety of options are available for biliary tract reconstruction. We present our experience of treating three children with extrahepatic biliary atresia by using appendix as biliary conduit. After mobilizing the appendix on its vascular pedicle, nonrefluxing, tunneled anastomosis was made with the 2nd part of duodenum and the appendix. The operative procedure is simple and less time consuming. From our preliminary experience with this technique, the operation seems simple and satisfying. The postoperative cholangitis was conspicuously absent. Though the long-term efficacy still remains to be proven, the appendix should prove durable as a functional conduit. Key words: extrahepatic biliary atresia, appendix. INTRODUCTION The use of intestinal segments to reconstruct the biliary system after surgery for biliary atresia is not new. Kasai et al1 first described Hepaticoportoenterostomy, which involved the use of a Roux-en-Y jejunal loop. Later, many modifications have been made in the technique by Kasai and others,2-6 but a major problem with these techniques has been ascending cholangitis. Ascending cholangitis has been noted in up to 50-90 % of cases with a high incidence of morbidity.7,8 The authors describe here their experience with the use of appendix as a Biliary conduit instead of jejunum for biliary reconstruction in three children with extrahepatic Biliary Atresia. The operation is easier and it achieves an anatomic reconstruction which is close to normal. MATERIAL AND METHODS Three patients with jaundice and acholic stools and hepatomegaly were referred to us were included in the study. The patient details are given in the Table 1. Clinical examination, and routine biochemical tests which confirmed the evidence of obstructive jaundice. An ultrasound of the abdomen did not show any intrahepatic ducts, nor was the gall bladder and the extrahepatic ducts visualized. HIDA scan was carried out in all the patients, which suggested no visualization of the gall bladder or extrahepatic ducts. The operative technique involves the dissection of the right colon and hepatic flexure so as to place the caecum under the liver. The appendix is then detached preserving the vascular pedicle. (Fig. 1) The caecum is closed in two layers. The tip of the appendix is cut open so as to form a tube from the appendix. This is then irrigated with solution of povidone iodine and saline. The caecal end of the appendix is then anastomosed at the porta with interrupted 5-0 dexon or vicryl sutures. The distal end of the appendix is then anastomosed to the duodenum after making a sub mucosal tunnel. (Fig. 2) The liver biopsy was suggestive of fibrotic biliary atresia with biliary cirrhosis. The postoperative period was uneventful in all the patients except for the onset of fever in one child which lasted for two postoperative days. There was no evidence of any sudden increase in jaundice, abdominal distension or positive blood cultures. All patients were discharged on the 8th to the 12th postoperative day. Post operatively, prophylactic antibiotics were continued for six weeks following the surgery in all the patients. DISCUSSION An ideal biliary conduit is one which should allow a free flow of bile from the liver to the duodenum, without allowing reflux of any intestinal contents back into the biliary tree. Though the jejunal loop is well known and effective, it has its own drawbacks. Cholangitis is one of the main problems that the surgeons have to face in these patients. As many as 50% of patients who have been operated for biliary atresia suffer from cholangitis. This high incidence has prompted various modifications of the jejunal grafts to prevent reflux e.g. using an interposition grafts, intussuscepted ileocolic interposition graft, 9-11 jejunal nipple valve 11-13, mucosal flap valve,14 and sphincter of Oddi valve15 but inspite of all these modifications the incidence of cholangitis remains significant. Postoperative cholangitis as suggested by Gupta et al 16 when appendix was used as a biliary conduit was possibly due to the role played by the presence of lymphoid follicles in the wall of the appendix. Jejunal loop has its own disadvantages i.e. the use of a wide loop which may necessitates tailoring, loss of a long jejunal loop out of the intestinal circuit. The use of the appendix on the other hand is well suited as a biliary conduit. The procurement of the appendix is simple and direct. The conical base and the tapering tip are well suited for biliary replacement in small children. The small caliber, well-vascularized isoperistaltic tube can be anastomosed to the duodenum using a nonrefluxing tunnel. The bile is directed into the duodenum, which is a physiological area for the intestinal and biliary contents to be mixed. We have had no febrile episodes to suggest Cholangitis in the two patients who are presently in follow up. The third child is lost to follow up and presumed to be dead. Follow up HIDA scans would be done after six months to assess the patency and the function of the conduit, but till then, lack of clinical evidence of cholangitis and increase in the intensity of jaundice has eliminated the possibility of reflux or strictures and ensured a free flow of bile. Currently in follow up patients are not free of jaundice, but the intensity has decreased considerably. Neither of the patients have signs of portal hypertension. Of late, this procedure has been reported to be used by some researchers for choledochal cysts and also in Biliary trauma.17 However, they suggest that it should be used only as a salvage technique when conventional hepaticojejunostomy repair is contraindicated.17 We have recently done a similar procedure in a 6 children with choledochal cysts, and the results are encouraging. The use of an appendiceal graft in biliary reconstruction was first reported by Grosfeld et al in mongrel dogs.18 Greenholz et al performed an ancillary appendiceal conduit to provide biliary drainage of an independent bile duct.19 Appendix has also been used as a ureteral conduit and long term patency and function has been documented for as long as 11 years postoperatively.20 Our initial experience with the use of appendix as a bilioenteric conduit seems to be promising. REFERENCES
Copyright 2002 - Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is02003f2.jpg] [is02003t1.jpg] [is02003f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}