 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 64, No. 6, Nov - Dec. 2002, pp. 502-505 Treatment of Breast Abscesses Using Systemic and Local Antibiotics Navneet Kaur Department of Surgery, University College of Medical Sciences & Guru Teg
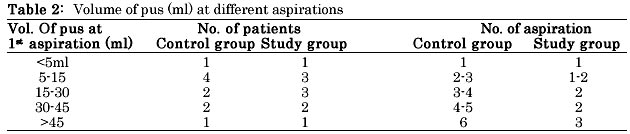
Bahadur Hospital, Delhi- 110095 Paper received: December 2001 Code Number: is02005 Abstract Local instillation of antibiotics has been shown to lead to faster healing in many deep-seated abscesses. A prospective controlled clinical study was carried out in 27 patients with breast abscesses to evaluate the effect on healing of local instillation of antibiotic into the cavity of breast abscess. In the control group (n=13), ten patients were managed by needle aspirations and three underwent incision and drainage of the abscess cavity. These patients received oral antibiotics. In the study group (n=14), ten patients were managed needle aspirations and four underwent incision and drainage. These patients, besides oral antibiotics also received antibiotics locally by instillation of injection Cloxacillin into the abscess cavity. Patients in the study group managed by needle aspiration had a significant reduction in healing time (5.4 days compared to 10.5 in control group, p < 0.05) as well the number of aspirations (1.8 compared to 3.4 in control group, p< 0.05). A significant reduction in healing time was also seen, when recovery time of patients in the study group managed by open drainage (5.7 days) was compared to patients in control group (17.6 days, p<0.05). None of the patients developed any complication as a result of the application of antibiotics. From this study, it can be concluded that local instillation of antibiotics besides systemic administration is safe and results in faster healing of breast abscesses. Key words: Breast, Abscess, Local antibiotics INTRODUCTION There is an ever-increasing search for therapeutic procedures that are convenient, cost effective and less invasive than conventional techniques. Patients demand procedures that minimize pain and trauma and have the least potential for side effects. Though incision and drainage under general anaesthesia remains the gold standard in the management of abscesses of the breast, less invasive procedures like incision and drainage and primary closure1 and repeated aspirations of the breast abscesses 2 have been tried and have shown variable results. A high local concentration of antibiotics achieved by local instillation in deep-seated abscesses has been shown to lead to faster healing.3,4 To evaluate the effect of local instillation of antibiotic, on the rate of healing of the breast abscesses, a controlled clinical study was carried out. MATERIAL AND METHODS Twenty-seven patients of breast abscesses presenting to surgical outpatients clinic over a period of 18 months at UCMS and GTB Hospital, Delhi were included in the study. In the control group (n=13), ten patients were managed by needle aspiration of breast abscesses and three by incision and drainage under general anaesthesia. In the group of patients managed by needle aspiration, the site of puncture for aspiration was anaesthetised by local infiltration of 1% lignocaine. The aspiration of the abscess was performed with an 18 or 19 gauge needle and as much pus as possible was aspirated. A sample of pus was sent for bacteriological examination. Subsequent aspirations were performed twice weekly till such time that no more pus could be aspirated. A detailed record was maintained of the pus drained at each aspiration and the number of aspirations required before complete healing was achieved. Remaining three patients were managed by open drainage under general anaesthesia. Of these, two had presented with clinically large abscesses and were considered unsuitable for needle aspirations. One patient presented with a chronic abscess following antibiotic therapy and underwent incision, drainage and curettage of the wall of the abscess cavity. All these patients received Cap. Cloxacillin 500 mg four times a day till the time abscess resolved completely. Patients with non-lactational breast abscesses also received metronidazole 400 mg three times a day. In the study group (n=14), ten patients were managed by needle aspiration. Two patients with clinically large abscesses and two with spontaneously burst abscesses underwent incision and drainage under anaesthesia. All these patients received oral antibiotics, as did the patients in the control group. They also received antibiotics locally by instillation of injection Cloxacillin into the abscess cavity. Prior to local instillation, all these patients were tested for any hypersensitivity to injection Cloxacillin. In the group of patients managed by needle aspiration, 500 mg of injection Cloxacillin reconstituted with 2-3 ml of distilled water was instilled locally into the abscess cavity after the aspiration of the pus. Local instillation was repeated at every subsequent aspiration. In patients with open wounds following incision and drainage of the breast abscesses, irrigation of the cavity was done with injection Cloxacillin at every dressing till the time wound was healed. All the patients included in this study were followed up at 1 and 3 months intervals for any residual or recurrent abscess. Lactating mothers were advised to continue feeding from the opposite breast and to express milk from the involved breast. Feeding from the involved breast was advised once the complete healing of the abscess was achieved. Statistical analysis was made between discrete variables by the student's t test. A p value of, <0.05 was considered to be significant. RESULTS The age of presentation was 19 - 42 years (mean 25.7 years). The mean age in the control group was 25.2 years and in the study group and in the study group 25.9 years. Twenty-three patients (85%) had lactational breast abscesses and 4 had non-lactational breast abscesses. In the non-lactational group two had developed the abscesses following FNAC for a breast lumps of tubercular mastitis, one in a young girl with retracted nipple and one in a patient with duct ectasia. Staphylococcus aureus was the organism isolated in 22 samples of pus and 4 were sterile. One sample of pus from the patient with duct ectasia isolated bacteroides supp. In the group of patients managed by needle aspirations, the mean volume of pus drained at first aspiration was 25.5 ml in the control group and 25 ml in the study group (Table 1). Hence the two groups were comparable in terms of the size of breast abscesses. Volume of pus at first aspiration and the number of aspirations required before complete resolution in the two groups are shown in table 2. The average number of aspirations required for complete resolution was significantly less in study group (1.8), compared to the control group (3.4) (p<0.05). The average duration of healing required was 5.4 days in study group which was significantly less than 10.5 days seen in control group (p< 0.05). In the group of patients managed by open drainage, the mean recovery time in study group (5.7 days), was significantly less than in patients of control group (17.6 days). A significant reduction in healing time was also seen when the mean recovery time of all patients in study (5.5 days) was compared to all the patients in control group (12.3 days) (p=0.001). In the follow up, only one patient managed by needle aspiration in the control group formed a small antibioma which subsequently resolved on conservative treatment. None of the remaining patients at follow up of 1 month and 3 months had any residual or recurrent abscesses. DISCUSSION Standard treatment of breast abscess is incision and drainage which requires a general anaesthesia, possibly an overnight stay in the hospital and regular dressings. In a lactating mother this causes considerable distress to both mother and the baby. In non-lactating breast abscesses, most of which are related to periductal mastitis, incision and drainage may be associated with recurrence and mammary duct fistula.5 In an attempt to reduce healing various less invasive methods of abscess drainage have been tried and have shown variable results. Jones and Wilson1 achieved a healing time of 6-8 days by the method of incision and removal of the wall of the abscess cavity under antibiotic cover. Azao et al6 achieved a faster healing time by instituting a negative suction drainage after incision and drainage and primary closure of the drained abscess cavity. Management of breast abscesses as outpatients by repeated needle aspirations has also shown good results.2,7 Ultrasonic guidance has proved to be a useful tool in assessing the adequacy of aspiration.8,9 We did not have access to ultrasound imaging for these patients, but 20 patients could be successfully managed as outpatients by needle aspirations. Concept of local instillation of antibiotics is not new. Florey et al 10 successfully treated small abscesses by daily aspirations and administration of large doses of penicillin into the abscess cavity. Local instillation of antibiotics has been shown to lead to faster healing in cerebral and pyogenic liver abscesses.3,4 In our patient too, the response to local instillation of antibiotics into the abscess cavity was dramatic. There is now no place for suppression of lactation in the management of breast abscesses. There are reports where breast feeding could be successfully initiated from the infected breast after drainage of pus.11 This leads to more effective decompression of breast and faster healing. However it is safe, if feeding is resumed 48 hours after drainage of pus and administration of antibiotics as this gives time for infection in the lactiferous ducts to settle down. Since most of the patients in this study were managed by needle aspiration, approach was more conservative and breast feeding from the involved breast was advised only after complete healing. Thus from this study it can be concluded that local instillation of antibiotic in the breast cavity is safe and effective and leads to faster healing as compared to the conventional methods. REFERENCES
Copyright 2002 - Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is02005t1.jpg] [is02005t2.jpg] |
| |||||||||

{kind=link}
{kind=link}