 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 64, No. 6, Nov - Dec. 2002, pp. 511-515 Preoperative Prediction of Survival in Oesophageal Atresia: A New Approach Pravin Kumar, Purnendu Ojha Newborn & Paediatric Surgery Centre, B-21, Patrakar Nagar, Kankarbagh,
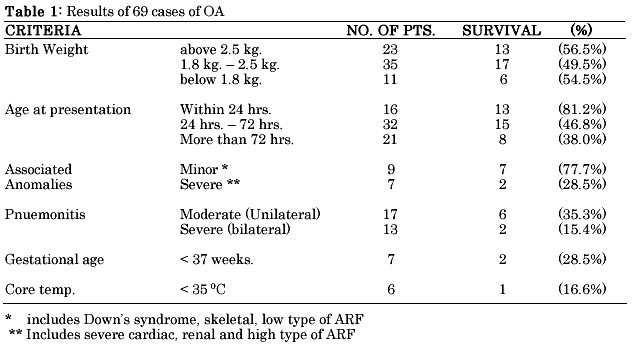
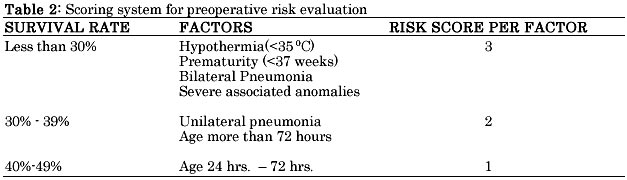
Patna 800020 Paper received: December 2001 Code Number: is02007 Abstract A retrospective clinical study to identify survivors from nonsurvivors in oesophageal atresia (OA) with or without tracheo-osophageal fistula (TOF) was done in a private pediatric surgery centre. During the seven year study period from 1992 to 1999, 69 neonates with OA / TOF were managed. The overall survival rate was 52.1%. Severe bilateral pneumonia, severe associated anomalies (cardiac, renal etc), prematurity and hypothermia were associated with poor outcome (survival rate less than30%). Moderate pneumonia (unilateral) and age of presentation of more than 72 hrs were associated with survival rates of 35.3% and 38% respectively. Birth weight was not found to have significant impact on outcome. A new scoring system for preoperative prediction of survival is proposed. Factors having significant impact on outcome were assigned risk score of 1 to 3 on the basis of their degree of impact on outcome. Neonates with total risk score upto 2 (low risk category) had survival rate of 82.1 %, which dropped to 7.1 % in neonates with total risk score of 5 and above (very high risk category). Survival rate of 44.4 % was observed in category with score of 3 - 4 (high risk category). We found this scoring system more accurate in pre-operative identification of neonates at poor risk for survival in our context than traditional Waterston's classification, which appears to have lost its usefulness. Key words: Oesophageal atresia, tracheo-oesophageal fistula, prognostic classification. INTRODUCTION Oesophageal atresia (OA) with or without tracheo-oesophageal fistula (TOF) is the most challenging problem in pediatric surgery. Waterston' s risk classification,1 traditionally used to identify neonates at risk for poor outcome has become obsolete in the developed world.2-4 Though various new prognostic classifications were proposed, none is applicable in our context as factors directly contributing to poor outcome in developing countries like India are different from those that exist in the developed world. Our experience in management of 69 cases of OA with or without TOF has been analysed and a risk evaluation system is proposed for preoperative prediction of survival. MATERIAL AND METHODS During the 7-year period from July 1992 to June 1999, 69 cases of oesophageal atresia with or without tracheo-oesophageal fistula were managed in a private hospital. A retrospective analysis of the medical records was undertaken. Parameters significantly affecting the outcome were identified. These included - gestational age, birth weight, age at presentation, core body temperature at presentation, associated congenital anomalies and severity of pneumonitis. An analysis was done according to number of patients and survivors in each group. A preoperative risk evaluation system was evolved on the basis of percentage of survivals (survival rate in each group). Factors associated with survival rate of less than 30% were assigned risk score of 3, those with survival rate of 30% - 39%, risk score of 2 and score of 1 was given for survival rate of 40% - 49%. No scoring was done for factors with survival rate of more than 50%. Regrouping of neonates was done according to risk score. Patients with risk score upto 2 were classified as low risk and with risk score of 5 and above as very high risk. An analysis was done according to number of patients and survivors in each risk category. RESULTS There were 44 male and 25 female neonates (M:F = 1.8:1). Average birth weight was 2250 gms. (Range: 1050 - 3200 gms). Mean age at presentation was 61 hrs. (Range: 3 hrs - 10.5 days). 36 out of 69 neonates survived postoperatively, an overall survival rate of 51.2%. Only 2 of the 7 preterm babies survived and one of the survivors was brought within 24 hrs of birth. There were 4 neonates with severe cardiac & renal anomaly (Fallot tetralogy - 2, PDA - 1, congenital multicystic kidney - 1) and all died postoperatively. Three neonates had high type of anorectal malformation. All underwent sigmoid colostomy as an additional procedure during same sitting and 2 out of 3 survived. Of the 4 cases with OA only, 2 died after cervical oesophagostomy and gastrostomy. 6 neonates had hypothermia at presentation, of which only one survived postoperatively. Hypothermia was more common in babies brought from remote place (4/6). Results of 69 cases are summarized in Table 1. Severe bilateral pneumonia, severe associated anomalies, hypothermia and prematurity were associated with poor survival i.e. survival rate of less than 30%. An inverse relationship between age at presentation and survival was noted. Birth weight was not found to influence outcome on its own evidenced by around 50% survival rate in all birth weight categories (Table 2). Twenty-eight neonates had total risk score upto 2 and 23 of them survived. Of the 27 neonates with total preoperative risk score of 3 - 4, twelve survived. None but one baby with risk score of 5 and above survived. The lone survivor was a preterm baby of 1600 Gms, brought to us after 80 hrs of birth, but was well preserved (risk score - 5). Survival rate in low risk category (risk score 0 - 2) was 82.1%, in high risk category (risk score 3 - 4) was 44.4% and was only 7.1% in very high-risk category (risk score 5 and above) (Table 3). DISCUSSION Waterston's risk classification1 used traditionally to identify neonates with OA with or without TOF at particular risk for poor outcome makes use of three factors - birth weight, severity of pneumonia and severity of associated congenital anomalies. Early diagnosis, improved surgical technique, neonatal anesthesia, sophisticated ventilator support, advanced intensive care management and early treatment of associated congenital anomalies have nullified the effect of Waterston's risk factors to a great extent. Improved survival rates were noted irrespective of Waterston's categories.2 In a historical review, Deurloo et al3 concluded that though the patients with OA treated now a days are born earlier, weigh less and have more associated anomalies than those treated 50 years ago, mortality rate is much lower due to early diagnosis, better supportive care and improved surgical techniques. In fact, Waterston's classifications have lost its prognostic usefulness and have become out dated in western world.2-5 In recent years new prognostic classification have been proposed. Montreal prognostic classification proposed by Poenaru et al4 suggested that only severe pulmonary dysfunction with preoperative ventilator dependence and severe associated anomalies have prognostic influence. Spitz et al5 observed that birth weight of less than 1500 gm and presence of major cardiac disease were the important predictor of outcome. Gidaro et al6 concluded that survival is related more to the presence of severe multiple associated malformations rather than bronchopneumonic complications of birth weight. Vagyu et al7 suggested that respiratory distress syndrome and pneumonia are still essential preoperative risk factors for OA. Recognizable chromosomal abnormalities like Down's syndrome and others has high mortality despite of treatment.8 Presence of right-sided aortic arch adversely affect - outcome by posing technical operative difficulties.9 Measurement of gap length was considered a simple and important predictor of survival in EA by Brown and Tam.10 These classifications may accurately identify survivors from non-survivors in centers where management of oesophageal atresia has been standardized but are not useful in developing world. Although, significant improvement in management and outcome of OA with or without TOF has been made in India during last two decades the survival rate of around 50% is still unsatisfactory. Two important reasons for unsatisfactory results are (i) delay in diagnosis leading to aspiration pneumonitis and septic complications and (ii) unsupervised transportation from long distances leading to hypothermia.11-14 Any prognostic classification not incorporating these facts can not accurately identify neonates at risk for poor outcome in Indian context, whether it be the traditional Waterston's classification or the modern Montreal classification. The reason that though we have achieved significant improvement in management of OA, most of the cases coming to us are in bad shape. In fact, we are away from Waterston but not near to modern western standards. Thus we require a risk evaluation system generated from our own Indian experience. The proposed system is an attempt to fulfill this requirement. The proposed risk evaluation system incorporates factors significantly influencing outcome in our context. Risk factors associated with most unfavorable outcome were assigned highest risk score. We observed poor survival (less than 30%) among neonates with hypothermia, prematurity, severe pneumonia and major life threatening associated anomalies. In a review of 341 cases of OA treated at All India Institute of Medical sciences (AIIMS), New Delhi, between 1980 to 1991, Bhatnagar et al observed similar survival trends in cases of these groups (12). Thus these factors were given highest risk score of 3. Birth weight was an important determinant of outcome in AIIMS Series but was not of significance in our series (Table - 1). This might be due to improved survival of low birth weight babies in recent past. As we observed around 50% survival rate in all birth weight categories this parameter is not included in our risk evaluation system as a risk factor for poor outcome. Age at presentation, not an important factor in western world, had inverse relationship with outcome in our series as well as others Indian series.11,12,14 Increased age at presentation mostly due to delay in diagnosis and sometimes due to delay in transportation to a pediatric surgery centre is a common occurrence in Indian subcontinent. Hypothermia, a usual outcome of unsupervised transportation in our part of world is associated with very poor survival but is neither a risk factor in traditional Waterston' s classification nor in modern classifications. Similarly prematurity which does not always lead to low birth weight does not find a place in prognostic classifications in common use, though it is a major risk factor in our series as well as most of the reported Indian series. The basic principle of proposed risk evaluation system is identification of factors having significant impact on outcome and assignment of risk scores to these factors on the basis of their degree of impact. Any centre involved in caring neonates with OA can evolve its own risk score, utilizing the principle of proposed system. This flexibility of system enables a pediatric surgical team to identify neonates with OA / TOF at poor risk for survival in their setups and thus will encourage them to put more efforts to improve survival in high risk and very high-risk categories. We found this system easy to use and more accurate in identifying survivors from non-survivors preoperatively than Waterston's classification. REFERENCES
Copyright 2002 - Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is02007t3.jpg] [is02007t2.jpg] [is02007t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}