 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 64, No. 6, Nov - Dec. 2002, pp. 516-519 Percutaneous Catheter Drainage of Liver Abscesses Sumit Kapadia, Dipesh Duttaroy, Pranav Ghodgaonkar, Sandip Maru Department of Surgery, Medical College and S. S. G. Hospital, Baroda- 390
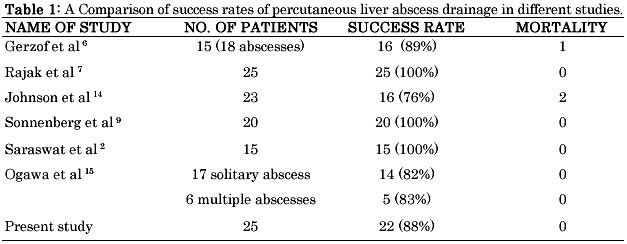
001, Gujarat Paper received: May 2002 Code Number: is02008 Abstract During a period of 32 months, 25 patients with liver abscess underwent percutaneous drainage under sonographic guidance - 22 had solitary abscess, while 3 had multiple abscesses. Pigtail catheters of various sizes were introduced in these patients using the Seldinger technique. The volume of pus drained ranged from 120 to 2500 ml, while the period of catheter drainage ranged from 6 to 38 days. Complications were minor and included catheter blockage in 3 patients, dislodgment in 3, tract pain and infection in 2 patients each. There was no mortality associated with this procedure. This study shows a success rate of 88% (successful treatment in 22 out of 25 patients). Hence this study confirms that percutaneous catheter drainage of liver abscesses is successful with a low morbidity and mortality and should be the first line of management in liquefied moderate to large sized liver abscesses. Key words: Abscess, liver, Amoebic, Pyogenic, Ultrasonography, Percutaneous INRODUCTION Liver abscesses, both amoebic and pyogenic, continue to be an important cause of morbidity and mortality in tropical countries. Although the primary mode of treatment of amoebic liver abscesses is medical,1,2 15% of amoebic abscesses may be refractory to medical therapy. Also, secondary bacterial infection may complicate up to 20% of amoebic liver abscesses.3 and hence drainage may be required in many patients with amoebic liver abscesses. Percutaneous drainage is now considered the treatment of choice for most intra-abdominal abscesses and fluid collections.4 The percutaneous catheter drainage technique is widely practiced by surgeons and radiologists alike. The present study evaluates ultrasonography (USG) guided percutaneous pigtail catheter drainage, assesses its response and evaluates the morbidity, mortality and complication rates of the procedure. MATERIAL AND METHODS This study was carried out in 25 patients with liver abscesses admitted to Shri Sayajirao Gaekwad Hospital and Medical College, Baroda during a 32-month period from July 1999 to April 2002. Of these, 24 were male and 1 female. Diagnosis of liver abscess was made on the basis of clinical history and examination followed by an USG. CT scan was not routinely performed. Abdominal pain (n=24) and fever (n=22) were the commonest presenting symptoms whereas jaundice with altered liver function tests was demonstrated in 4 patients. Elevated total white blood cell count (WBC count > 10,000/cumm) was found in 3 patients (12%). Hematological investigations which included bleeding time, clotting time and prothrombin time were performed in all the patients and were found to be within normal limits. USG showed involvement of right lobe in 21 (84%), left lobe in 1 (4%) and involvement of both lobes in 3 (12%) patients. Serological tests, which are often performed for diagnosis of amoebic liver abscesses were not performed in any of our patients due to their unavailability in our hospital and financial constraints. A chest x-ray was performed in all the patients. Indications Indications of catheter drainage included large sized liquefied or partially liquefied liver abscesses (>5 cm diameter) refractory to medical line of management. Technique Catheter drainage was performed using the Seldinger technique as described in the literature6 as a joint effort between the surgeon and the radiologist. Injectable atropine 0.5 mg was given intramuscularly half an hour before the procedure. Abscess was localized by USG and a safe drainage route planned to avoid the bowels and costophrenic recess. Under all antiseptic precautions, the site was marked and infiltrated with 2% lignocaine. A 4 mm stab incision was made through which an 18 G guide wire introducer needle was passed under sonographic guidance till it reached the center of the cavity. A guide wire (Cordis 0.038, Johnson and Johnson) was then introduced through the needle and positioned inside the cavity following which the needle was removed keeping the guide wire in situ. Serial dilators (Devon Ltd.) were then passed over the wire to dilate the tract. The tract was dilated to an adequate size depending upon the viscidity of the pus. A pigtail catheter of size smaller than the last dilator was passed over the wire and positioned in the center of the abscess cavity under sonographic guidance. The guide wire was then withdrawn and the pigtail catheter was connected to a closed drainage bag and fixed to the skin. Sterile dressing was applied. The pus was sent for aerobic culture. The daily output was monitored. The catheter was flushed daily with 10 ml of normal saline to prevent its blockage with debris.7 Metronidazole, ciprofloxacin and gentamicin were given in therapeutic doses for a period of 2-4 weeks. Alternate day USG studies were done to monitor the cavity size and volume and to confirm the position of tip of the catheter. Clinical improvement in the patients' condition was noted. The pigtail catheter was removed when drainage become serous and it either ceased or was minimal (<10 ml in 24 hrs) and USG was suggestive of reduced size / collapsed cavity without any residual pus.2 A cavitogram study was done by instilling 20 ml of contrast dye (diatrizoate) through the pigtail catheter in 4 patients in whom there was persistent drainage of bile stained pus. On removal of the catheter, sterile dressings were applied. All patients were called for monthly follow up and were assessed clinically and ultrasonographically. RESULTS Twenty-five patients of liver abscesses more than 5 cm in size underwent USG guided percutaneous pigtail catheter drainage. The duration of symptoms ranged from 7 to 30 days. 22 patients had single abscess while 3 had multiple abscesses. Most of the abscesses were liquefied or partially liquefied on presentation (n=22) while 3 were not liquefied on presentation. The size of the abscesses ranged from 5 to 18 cm in diameter. Abnormality in X-ray chest was seen in 2 patients. One had a right sided empyema which required intercostal drainage, while the other patient had a raised right hemi diaphragm due to a 9 x 7 cm sized abscess in segment VII of liver. Catheter drainage achieved good symptomatic control in all the patients within 48 to 72 hrs, while the leucocytosis came back to normal within 5 to 9 days. The serum bilirubin levels came back to normal within 7 to 10 days in the 4 patients with jaundice. The range of catheter duration was 6 to 38 days with an average of 14 days. 4 patients had persistent bile stained discharge (due to cavity communicating with the biliary tree), which required prolonged drainage but ceased on its own. Aerobic culture was positive in only 2 patients and showed a growth of Klebsiella in both. Anaerobic culture was not performed. The total amount of drainage of pus from the cavity ranged from 120 to 2500 ml, with an average of 787 ml. Complications of percutaneous drainage were minimal. They included catheter blockage (n=3), catheter dislodgment (n=3), tract pain (n=2) and infection (n=2). The catheter blockage was managed by regular flushing of the cavity with normal saline. Dislodgment required replacement of the catheter under sonographic guidance, while the pain and infection responded to analgesics and antibiotics respectively. There was no mortality associated with this procedure. In our series, the treatment was considered successful if all the following criteria were met: clinical improvement, normal WBC counts, USG suggestive of total resolution / reduction of cavity size to < 3cms and there was no evidence of relapse / recurrence on follow up. 7 Based on these criteria, 22 patients were treated successfully, 2 had recurrence and 1 was lost to follow up. Out of the 2 patients with recurrence, one was asymptomatic but was found to have a 5 x 5 cm sized cavity in the right lobe on USG follow up. He responded to oral metronidazole given for 2 weeks. The other patient was symptomatic and had an abscess cavity of 6 x 5 cm 4 months after follow up. He underwent a repeat pigtail catheterisation with medical management for 15 days to which he responded. The success rate for this procedure is 88% (22 out of 25), which compares well with the other studies depicted in Table I. DISCUSSION Percutaneous treatment (needle aspiration or catheter drainage) is now a standard management for liver abscesses.6-10. It has replaced surgical exploration which now has very limited indications. Needle aspiration is less expensive, avoids problems related to catheter care and long-term hospital care. Multiple abscesses can be aspirated through different tracts in the same sitting. However, needle aspiration has lower success rate than catheter drainage.7, 8 Another problem with aspiration is that repeated needle aspirations (average number per patient ranging from 1.4 to 5) may be required in a single patient over a short period of time from 5 to 14 days.7 This may be painful and unpleasant for the patients and hence may not be acceptable to them. To avoid these problems associated with needle aspiration, percutaneous pigtail catheter drainage is now used as the first tool in the management of liver abscesses. The advantage of catheter drainage is that it provides a continuous outlet to the pus and hence the problems of incomplete and repeated evacuations are not encountered. Therefore this procedure has a high success rate reported in the earlier studies and also in this present series (88%). The problem of failure of this procedure as reported by earlier studies 9,10 has been due to the thick and viscid pus, which cannot be easily drained by percutaneous drainage or early premature withdrawal of the catheter. These problems can be avoided by using adequate sized pigtail catheters depending on the viscosity of pus (5 Fr. to 12 Fr.) and following a strict protocol for catheter flushing and removal. One of the major problems is a prolonged duration of the catheter. This led to some authors considering this procedure as slow.11 Another important factor to be considered is the cost factor. A single procedure would cost the patient an additional 300 rupees over and above the cost of the reusables costing 1500 rupees. However looking to the advantages, the financial burden to the patient or the hospital would be justified. Sonographic resolution of an abscess cavity following this procedure may occur at any time between 2 weeks to 4 months.12, 13 Small residual cavities may persist indefinitely. 40 % of our patients had small residual cavities (< 2 cms) at 3 months of follow up. Percutaneous catheter drainage is a safe procedure with very few reported complications6,9,14 which includes hemorrhage, perforation of hollow viscera, peritoneal spillage, catheter displacement or blockage and septicemia. But recent studies show very low complication rates.2,7,12,15 Our study did not have any major complication although the incidence of minor complications was 40 % (10 patients). The chief limitation of our study is that patients with amoebic and pyogenic liver abscesses could not be segregated due to the nonavailability of serological tests. However, without a firm and specific diagnosis, the abscesses were drained in the belief that percutaneous drainage would cure a pyogenic abscess in a shorter duration and in case of an amoebic abscess would hasten the patients recovery. To summarize, percutaneous pigtail catheter drainage is a safe and effective mode of treatment of liver abscesses, both amoebic and pyogenic. It results in an early relief of symptoms and faster resolution of abscess cavity. The low morbidity and high success rate in treating liver abscesses, which otherwise would have a fatal outcome if untreated, by this minimally invasive method suggests that this therapy should be the first line of management in liquefied moderate to large sized liver abscesses. REFERENCES
Copyright 2002 - Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is02008t1.jpg] |
| |||||||||

{kind=link}