 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 64, No. 6, Nov - Dec. 2002, pp. 529-531 Case Report Multiple Recurrent Fibroadenomas in a Nulliparous Adolescent Female - Treatment Difficulty Yamaç Erhan,1 Hasan Aydede,1 Aslan Sakarya,1 Mine
Can,3 Ali Emre Atýcý,1 Departments of 1 Surgery,2 Pathology and 3 Radiology,
Celal Bayar University Medical Faculty, Manisa, Turkey
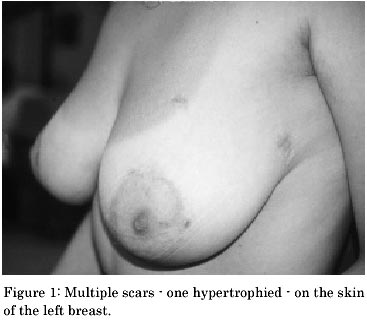
Paper received: April 2002 Code Number: is02013 Abstract Fibroadenomas comprise most of the benign breast lumps among young females and present as well circumscribed masses in the breast. Multiple fibroadenomas are not uncommon. But the presence of more than four fibroadenomas in one breast with recurrences at different time periods is rare. A case of multiple, bilateral and recurrent fibroadenomas (12 previously excised lesions, 17 gradually formed fibroadenomas during follow-up) in a 22-year-old nulliparous female who is still on clinical follow-up is presented. This unusual case is helpful to enlighten the difficulty which may take place in the management of such kind of recurrent multiple fibroadenomas of the breast in the adolescent nulliparous female. Key Words.: Fibroadenoma, mastectomy, biopsy, FNAB, ultrasonography INTRODUCTION We present a case of multiple, bilateral and recurrent fibroadenomas in a 22-year-old female with a family history of breast cancer who is on clinical follow-up. CASE REPORT A 17-year-old University student first presented in July 1996 with a month history of bilateral non-tender breast lumps. Her mother was treated for carcinoma of the breast in 1985. She had never taken oral contraceptives nor had she been pregnant. Menarche was at 12 years of age. Examination showed the presence of 4.2 cm lump in the right breast and two other 2.7 and 2.5 cm breast lumps on the left breast. Histology revealed them all to be fibroadenomas with delicate fýbroblastic stroma, varying in cellularity from lesion to lesion, enclosing slit-like or tubular structures lined by a bland-looking epithelium. She returned approximately 2 years later with a hypertrophic scar, 4 mobile lumps on the right breast and 5 mobile lumps on the left side in different quadrants, all clinically suggestive of fibroadenomas on physical as well as ultrasonographic examination. These two lumps bigger than 2 cm were treated with excisional biopsy using previous scars and a new incision. Histology of all these excised lesions showed them to be fibroadenomas. A clinical decision of annual observation policy was taken and the patient was taught for self examination of the breast. In August 1998, the patient again presented with newly found non-tender breast lumps feeling the anxiety of breast carcinoma even though the clinical situation was detaily explained her. Two new masses which were clinically palpable, 1.2 cm in the right and one 1.5 cm in the left breast were detected by ultrasound. Hormonal assays including plasma estradiol and progesterone levels were normal. FNAB of the masses confirmed fibroadenomas. Surgery was not recommended to avoid multiple unpleasant scars and the structural distortion causing difficult ultrasonographic follow-up unless the lumps were bigger than 2 cm. In August 1999, the patient was seen regarding new bilateral breast masses that she discovered herself. Two new mobile masses on the right and one new mass on the left, the biggest 10.9 mm by ultrasound, were found in addition to the previous ones which remained almost in same dimensions. FNAB confirmed the biggest masses as fibroadenomas. All of these 11 masses smaller than 2 cm were decided to be observed. In February 2000, one additional mass, 2 cm in dimension, in the right breast and two additional masses, 11.2 mm and 11 mm in dimensions, in the left breast were found. Four of the previous lumps which remained unchanged before were found slightly bigger on the last examination (2 in the left and 2 in the right breast). FNAB again confirmed fibroadenomas. All of the four previous masses bigger than 2 cm with the newly found 2 cm mass were removed by using previous scars (Fig 1). Histologies of the lesions were fibroadenomas and immunohistochemistry were negative for p53 and Ki-67. In June 2000, three new masses in the left breast (6.5 mm, 6 mm, 12.5 mm) and two new masses in the right breast (5.5 mm and 13 mm) developed. Since the fibroadenomas became recurrent, she was recalled for clinical examination three months later. In September 2000, ultrasonography revealed two more new masses additional to the ultrasonographic findings of June 2000, 11.5 mm in the left breast and 7.5 mm in the right breast upper. Some of the other masses found on June 2000 were slightly bigger. The patient also complained of left mastalgia, although there was no objective change in the breast morphology and advised to take analgesics for breast pain. On February 2001, there was a new small fibroadenoma clinically nonpalpable but ultrasonographically detected in the left breast.The ultimate total number of fibroadenomas present in both breasts were 17.But some of the lumps were slightly bigger than before and the biggest fibroadenoma was 18.3 mm. We recommended the patient self examination and close clinical follow-up. DISCUSSION Usually one or two fibroadenomas occur in a patient, but bilateral lesions or even up to four in a single breast is a relatively common feature.2 The great majority of fibroadenomas are histologically and clinically similar to the slow-growing "adult" fibroadenoma seen in older women.1 Less than 5% of fibroadenomas have the clinical and histologic characteristics of giant fibroadenomas defined as either having a diameter greater than 5cm and / or a mass heavier than 500 gm.4 Multiple fibroadenomas and especially recurrent cases have been reported very rarely and the majority of these cases have been part of familial syndromes, in non-Caucasian women.3 Our patient is Caucasian, has one unaffected sister and has a family history of breast cancer. There are available data about its strong familial connection in most of the reported cases, but this has not been proven for non-multiple lesions.3 Oral contraceptives are thought as having a possible role in the aethiology by some authors.5 But despite this report, our patient had never taken oral contraceptives nor been pregnant. There are also some authors who have failed to find a link.6 The suggestion about the ideal treatment of such cases is controversial. There are no reports to detail the benefits of antiestrogens in juvenile fibroadenoma. Some authors advocate local excision of the individual lesions as they appear with emphasis on preserving sufficient breast tissue, but this could lead to undesirable scarring, especially in young patients with a tendency to formation of hypertrophic scars.7 This problem showed itself in our patient with several scarring in her breasts although we tried to excise some of them utilising the mobility of fibroadenomas through a single cosmetic circumareolar incision in each breast as it was previously described by Naraynsingh and Raju.8 But this approach could lead to extensive duct damage. Multiple lesions have also been treated conservatively as has been suggested for single lesions because they have, in fact, benign cytologies and typical clinical and ultrasound appearances. 3, 9,10 Recurrent cases, large fibroadenomas, multiple scars causing breast deformity as a result of repeated excisions and having the experience of physical and emotional discomfort from this condition would bring subcutaneous mastectomy with reconstruction as a logical solution for bilateral and diffuse breast involvement.11 From another point of view, there are nearly 100 documented cases of carcinoma arising within the epithelial componenet of fibroadenoma12. These data exclude cases of cystosarcoma phylloides and cases in whom a fibroadenoma is secondarily infiltrated by an adjacent carcinoma. As frequent recurrences of her fibrodenomas, enlargement of the previous ones, multiple scars resulting in breast deformity and her family history of breast cancer, we recommended this young and nullipare patient close clinical follow-up In conclusion, this unusual case is helpful to enlighten the difficulty which may take place in the management of such kind of recurrent multiple fibroadenomas of the breast. REFERENCES
Copyright 2002 - Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is02013f1.jpg] |
| |||||||||

{kind=link}