 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 65, No. 1, Jan.-Feb. 2003, pp. 30-37 Perspectives of Rural Surgeons Organising a Rural Nursing Home R. D. Prabhu Shree Dutta Hospital, Tilak Nagar, Shimoga-577 201 Paper received: June 2002 Code Number: is03005 Abstract Rural India needs more surgeons In order to practise, of them will need to construct their own nursing home. But the technical information on the minimum standards and requirements in such nursing homes is not easily available. Many simple ideas help lower the construction costs and good planning can help efficient use of available space and funds. Some governments have laid down minimum standards for nursing homes, which if not complied with may land the surgeon in trouble with the law. It is also important that the surgeon is able to offer good affordable treatment and comfort to the rural patient. Key words: Rural nursing home, area per bed, rural operation theatre. INTRODUCTION A surgical nursing home in rural India has to be able to manage primary and secondary care of a patient. Any surgeon who wishes to undertake such work in a rural, taluka or district place needs to satisfy himself, that the venture will be feasible in the chosen community. It is reported that in Africa, for every 1000 patients who attend a primary care centre, about 50-100 need secondary care 1. Though this condition may not apply to India, a rural nursing home in India must be located in an area accessible to a large number of people. The Bureau of Indian Standards (B.I.S.) has published a booklet on Basic Requirements for Hospital Planning 2. But those requirements are virtually impossible for most of the rural surgeons for example a 30 bed hospital needs an acre of land, 1800 M2 (1936n sft.) of built-up area, 240 M2 (2582 sft.) for an Operation Theatre cum Labour Room suite, 2 employees per bed to be increased to 3 per bed, once the nursing home works to full capacity, etc. etc. However, the booklet is a useful guide as far as the requirements of instruments and equipment for a nursing home are concerned. The following information has been gathered from different sources and is presented here. Rented Building The wiser ones decide to start their practice in a rented building and if they succeed then take up the construction of a nursing home built with a purpose rented building is a very economical way of starting practice. However, it has many difficulties. First of all it is very difficult to find a building large and suitable enough for a nursing home, even if the consultation rooms are in a separate house. Most of the buildings are built for residences and the number of rooms and their layout is not suitable for a nursing home. It may not be possible to separate the clean and unclean sections of the nursing home the sizes of rooms are usually not adequate and none of the rooms are large enough to accommodate an operation theatre. The doors are too small for a wheel chair to pass through and the passages too narrow to negotiate a stretcher trolley. If one has to utilize the first floor of the building, transporting a patient there becomes difficult. However, in spite of all this with some alterations in the building and with some compromises, one may be able to set up practice for a few initial years or at least until one is convinced of good future prospects. A Nursing Home built with a purpose: The planning of a nursing home is a vast subject and it may not be possible to cover all its aspects in a small article like this. The engineers and architects in small towns are not aware of the needs and specifications of a small nursing home. So some general principles and guidelines are being discussed so that the surgeon may be able to guide the design of his own nursing home. The surgeon may not be able to satisfy all these principles, but they will certainly help a good architect in designing a master plan so that difficulties are minimized. The main constraints of a rural surgeon are :3
In the initial stages it is advisable to opt for flexible and low-cost designs till one
is sure of the local needs. A rapid increase in
the Site for the nursing home Having decided on constructing a nursing home, a suitable site has to be found for it. Ideally the site should have the following features.
The Building The general considerations: A building is valuable asset though the construction cost is only a fraction of the running cost over a period of fifty years, the normal life of a building.6 A properly planned construction will certainly reduce the cost of construction and improve the efficiency of functioning. Availability of land is easy and land is affordable in a rural place, therefore one level (ground level only) construction with load bearing walls and horizontal extension is more economical. If the land available is small then vertical extension with pillars and beams is ideal. Vertical extension needs a lift or a ramp. Lifts are, not only costly to install but also costly to repair. They need expert maintenance and continuous power supply. A ramp is a very good alternative, convenient and comfortable. The ideal gradient for a hospital ramps is 1:10. One need not incorporate all high-tech facilities at the very beginning. Very good surgery can be performed with basic facilities.
Civil Planning It is always advisable to draw a master plan for the present and future requirements of the nursing home. The nursing home itself must have the following minimum facilities.
Some of the states in India, like Karnataka, have already laid down certain minimum standards for private nursing homes (Karnataka State Nursing Home Ordinance 1975/Act). In these states their norms have to be followed. There are WHO standards, western (W), B.I.S.2 and Indian (I)9 standards available too; but all may not be suitable for small nursing homes. Indian values are mostly for large general hospitals. Where there are no hard and fast standards laid down, one may consult a practicing rural surgeon in the field and also use whatever information that is available to develop a more practical approach. 1. Outpatient section Requirement of total area for outpatient section :10M2 (about 111 ft.) per bed.10 The purpose of the outpatient section is to receive patients, investigate and diagnose their ailment and then, either treat and send them home or admit them to the hospital for further management. This section need not be a part of a nursing home, it may be separate and even elsewhere in the town. But having both out-patient and in-patient facilities in one building is always convenient, economical and leads to better utilization of manpower. The consulting doctor is available for in-patient care too. The outpatient section must have the following facilities. a. One or more consultation rooms. Consultation Room area requirement : Though the surgeon may start his practice alone, very soon he is likely to have a partner -m a physician, obstetrician or even an anaesthetist to help him out. The Karnataka Government expects two doctors for bed strength of up to 25. So a second consultation room will be useful. Later, when the practice is established, the rural surgeon may extend his services by inviting specialist practitioners to visit this nursing home. One must make a provision for adding more consultation rooms for them in future. Usually a 10 ftx 10 ft room may be adequate for consultation; a larger room is more comfortable. Having a separate room for examination of the patient is very convenient. A basin with a hand wash is useful in each consultation room. b. The waiting room must be large enough (KG-100 sft) to accommodate the waiting patients and their relatives comfortably. If it is centrally located it must be of a larger size since it serves as the waiting room for other facilities like laboratory, treatment room or even dispensing room. Comfortable seating and adequate number of toilets must be provided. c. A treatment room (KG-120 sft). d. One needs a small clinical laboratory for basic investigations like the examination of urine haemoglobin estimation etc. However, it must have a provision for the introduction of other equipment for special investigations in future. e. It may be useful to have a small room with a dispensing counter from where essential and emergency medicines can be dispensed. f. One may make a provision for future extension of the department for newer technologies like ultra-sonology, endoscopy, radiology etc. 2. In-patient section One must plan for at least ten beds and to be cost-effective, about twenty to twenty-five beds, less than ten beds is not cost-effective and more than twenty-five need more than two doctors in attendance (Karnataka Govt. Ordinance / Act) . It is also said that on an average one needs one operation theatre per 25 surgical beds (or 50 general beds),11 Floor space requirements per bed Wards :
Single- bedded rooms :
The general considerations are as follows:
3. Operation Theatre suite
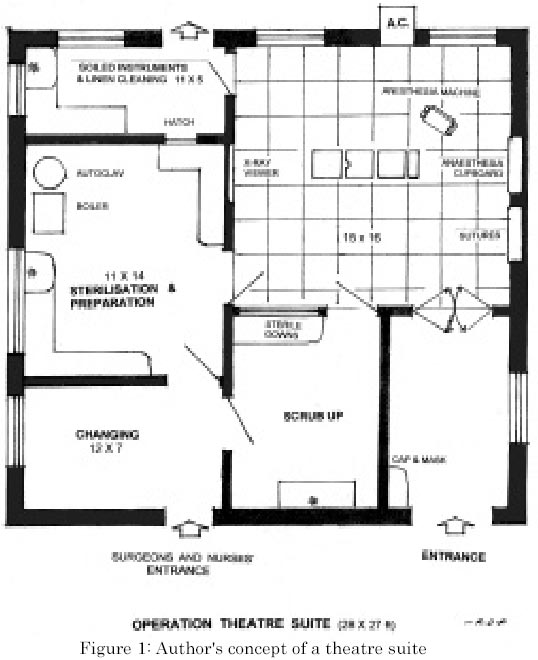
This is a vital part of a surgical nursing home. Information available in the literature is such that any amount of investment may be made in it and still be considered insufficient. The surgical work in a rural nursing home being mainly secondary care work, one can manage with simple furniture and equipment to start with and then add more costly ones in due course of time. ( Fig 1 ) The suite needs:
The operation theatre floor and walls must be waterproof, dustproof and washable, stainless steel sheets for the walls are seen in western operation theatres, but for us stone, marble or ceramic tiles serve well. Many have painted the walls with enamel washable paint! Corners and junctions in walls, floors and ceilings must be rounded off to prevent accumulation of dust and to facilitate cleaning. Unavoidable anaesthetic cupboards and wall mounted panels, view box, etc. may be recessed into the walls to prevent injury to personnel moving around the operating team. Provision for a wall-mounted air conditioner may be made where the climate of the area demands it. It is advisable not to have any storage shelves inside the operation theatre: shelves collect and store dust. Air from the wards may be prevented from entering the operation theatre suite. Similarly, the door to take away the used and dirty articles from the operation theatre should lead to a separate cleaning area. The Operation table is one of the most costly equipment of this room. Primarily, an operation table should a) support the heaviest of the patient, b) be movable and easily cleaned, c) quickly give head low position and d) have provision for lithotomy position. Many a successful rural surgeon has started his practice with a fixed height, mechanically operated table in the initial stages. There are some that have used them all their lives. Only when there are many surgeons who need varying heights of the table, or need side tilts etc. will the necessity of a multiposition table whose height can be increased or decreased arise. An operation light is a vital accessory for comfortable surgery. Shadowless, cold, ceiling lights are preferable. A suction apparatus, which can create a negative pressure of about 30 lbs p.s. i is essential to aspirate thick mucus and blood clots. Another equipment that is handy is a simple diathermy unit. Each surgeon has his own preference for certain surgical instruments. It is best that a surgeon buys a basic general set of instruments, in addition to his preferred special instruments (like scissors, needle holders, etc) to start with and then goes on adding the required instruments in stages. Indian manufacturers do not always respect the specifications for surgical instruments. Unfortunately there is no official body in India that checks the quality and calibrations of health care equipment. Hence it is advisable to inspect each item individually before making the purchase. A single-drum autoclave from a reputable manufacturer, and operated with external heat is adequate in the initial stages. It is found that a single-drum autoclave cycle is shorter and hence damage to the heat sensitive articles is less, and using it again after one cycle reduces the time of the subsequent cycles even further. Anaesthetic equipment has to be purchased in consultation with the anaesthetist of the nursing home When there is no qualified anaesthetist to help; the surgeon, many rural surgeons have start ed with the basic, Rao's draw-over' bottle for simple air + ether anaesthesia. An Ambu bag must be kept handy. E. M. O. (Epstein and Macintosh, Oxford) machine is a sophisticated yet simple to handle version of a draw-over bottle. But there are not many anaesthetists nowadays who are conversant with this apparatus. Anaesthetists now need a Boyle's apparatus. So the surgeon must start making a provision to buy one sooner than later. There must be sufficient number of oxygen and other anaesthetic gas cylinders. If refilling is done far away additional cylinders will be necessary to supply the gases until refilled ones return. It has been confirmed by WHO that industrial oxygen is harmless for human use. Standard anaesthetic accessories like the laryngoscope, endotracheal tubes, drugs etc. may be kept ready in consultation with an anaesthetist. Depending upon the anaesthetist, the surgeon may have to buy other accessories of anaesthesia like a) pulse oxymeter, b) monitor, c) ventilator, etc. A room air-conditioner set in the wall of an operation theatre is for the comfort of the operator. It is not a necessity for the aseptic work, in fact in many a theatre where there was bad outbreak of infections like tetanus, the source of infection was traced to the air-conditioners. Central air-conditioners are very costly to install, and they too can be the sources of infections. Spark-free electric switches for operation theatres have been recommended. However, a vast majority in India has installed ordinary switches and one is not aware of any catastrophes. It is better to have windows for an operation theatre. Air outside is cleaner than the one inside the nursing home, except when there is dusty wind blowing outside. Keeping the window open exchanges the polluted theatre air for fresh air, which is relatively purer. There must be provision in the windows for tinted or opaque shutters, to reduce the incoming light for special procedures like endoscopies. An Intensive Care Unit for post-operative care is indeed an ideal thing but needs heavy investment . However, the most important part of an ICU is the trained staff and not the gadgets. If one has well-trained staff in a rural nursing home, they can look after a majority of operated patients even without any special gadgets. When funds permit, the addition of these gadgets will improve the efficiency of the same staff. Special Equipment The need for special equipment must always be weighed against a) viability of the investment and b) easy availability of good service engineers. It can be very frustrating when costly equipment cannot be used for long periods for want of a service engineer to repair and calibrate it. Sometimes equipment that enhances the practice may have to be purchased though the actual returns from it are not adequate for example, additional gadgets in an operation theatre. On a rough estimate, it is believed that any special equipment must be able to earn at least a quarter of its cost per year to make the investment cost-effective. One must also remember that complex functions of complex machines can be accomplished only if one has efficient, qualified personnel to operate them. With unskilled labour, simple and foolproof techniques and solid and safe equipment is preferable. X-Ray machine : If this is considered to be essential, one will have to have a separate room for it. It will also need a good dark room for the processing of the exposed films. To reduce the hazards of radiation to people around the room, the walls must be made of 8-12 cm thick concrete, which is equivalent to a mm thick lead sheet or 5 mm thick steel sheet. The outer wall may be of usual brick and mortar but then no one must be allowed to go within 3 ft of it 16. Water supply Nursing homes need a large volume of good soft water, about 140-180 litres per patient per day. It is advisable to make a provision to store water that is twice the daily requirement. Not every place has a good water supply. Hard water damages the instruments and delicate equipment. This difficulty can be overcome by installing a small water-softening unit in the distribution circuit Waste disposal and prevention of pollution A recent enactment has made it mandatory that all health care units take all the steps to prevent pollution of air and water and to destroy biomedical waste. The surgeon has to apply for permission from the State Pollution Board to run a nursing home, and then make arrangements to dispose the biomedical waste in the manner prescribed by the board. Amongst the unavoidable requirements, the incinerator is the costliest equipment (Rs.15-20 lakhs!) that a surgeon may have to invest in and is expensive to operate as well. A good incinerator is one that burns the material at a very high temperature (around 18000C ) and washes the effluent gases coming out of its burning chamber. Disposal of plastics like syringes, parenteral fluid bottles, drip sets, etc is a problem too since they all need to be crushed so that they are not reused. Besides, chlorine-containing plastics are not supposed to be incinerated; they produce extremely dangerous dioxins when burnt. These poisons affect the genes of the adults and show morbidity in future generations! It would be ideal if local governments take over the responsibility of installing common, safe and efficient incinerators. Legal requirements In addition to the laws governing the hospital setting, one also has to comply with Minimum Wages act, Labour laws and the Employee's Provident Fund rules. Unfortunately, most of these rules attract Criminal proceedings in case of default! CONCLUSION Starting a surgical nursing homes in a rural place is quite exciting and adventurous. Each surgeon must first find a community that accepts him best. Until his future prospects are assured, it may be wise to start a practice in a rented building despite all its disadvantages. Once the surgeon is sure of his practice, he may venture to build a nursing home with a purpose in stages. It is always wise to satisfy the technical requirements of a nursing home during the initial construction itself, alterations later are cumbersome and costly. In the private sector the investment must take into consideration the economic status of the community it will serve. All along one must try to see that one is working within the framework of current laws. REFERENCES
Copyright 2003 - Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03005f1.jpg] |
| |||||||||

{kind=link}