 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 65, No. 1, Jan.-Feb. 2003, pp. 50-54 Surgical Training Distance Education--A Training Tool for Rural Surgeons Tapan K. Jena, Ashok K. Agarwal The School of Health Sciences, Indira Gandhi National Open University, New
Delhi-110 068. Paper received: July 2002
Code Number: is03010 The concept of Rural Surgery has developed during the past few years to make basic limb saving and life-saving surgery available within limited resources for those who have no access to it under their present socio-economic circumstances. Hafden Mahler, Ex-Director General of WHO labelled this type of care as 'Essential Surgical Care'. Indira Gandhi National Open University (IGNOU) has tried to translate this concept into an academic exercise with an objective to materialise the concept of 'surgery at doorsteps.' For a better understanding, the term 'Rural Surgery' may be defined as the practice of need-based multidisciplinary surgery under resource constraints to make surgical care affordable and accessible to the community. COMMUNITY NEED IN SURGICAL TRAINING The very basis of university education has been to cater to the needs of the community taking into account its cultural considerations. We know that culture is an outcome of social adaptability for its self-reliance. Therefore, the future need and practice of surgical care in a given country should be determined in the light of its sustainability as a caring system. In a developing country like India, where per capita annual income is about 500 US$, where there is no operational referral system, where there is no fixed area responsibility for surgical care and where facilities for transportation are meagre, a surgeon has to be well trained to handle all types of surgical emergencies under various resource constraints; be it in terms of manpower, equipment or infrastructure. Moreover, the practice of appropriate technology, wherever essential, with a combination of local innovations and adaptations could not only make the surgical care affordable and sustainable but also accessible. All these could be achieved without compromising on quality if we take a fresh look at the training system and redesign it keeping the needs of the community at the focus of our academic planning and design. COMMUNITY CONSIDERATIONS IN TRAINIGN DESIGN The prime consideration for any community-based care should be its accessibility by rural masses. When a patient with a surgical emergency has no access to a tertiary superspeciality centre, the solution may lie in transferring the essential surgical skills to the remotest area without compromising on the quality of the service. The spectrum of multidisciplinary practice being done by the rural surgeons1 is an indicator for deciding the type of surgical training that could be provided to rural surgeons. Indeed, this type of input from time to time could help in modifying the training package for rural surgeons that would be both time and country specific. The morbidity and mortality pattern in India indicates that any rural surgical training of this nature should at least include the disciplines of general surgery, Orthopaedics, ENT and Obstetrics and Gynaecology. In present-day practice no surgery can be organized without the help of anaesthesia and radiology. Surgery being a team effort, paramedical training, hospital administration and finance form other important considerations. With the increase in longevity and the consequent changes in the pattern of morbidity, the management of long-term illnesses including malignancy, necessitates another dimension of training for rural surgeons. The fact, however, remains that a multi-skilled surgeon should be aware of his limitations and that he has a moral responsibility to guide for appropriate referral, as and when required. DISTANCE LEARNING AS AN ACADEMIC TOOL Distance education has emerged out of the human need to learn amidst all types of constraints and adversities. The system is not only an excellent blend of flexibility in terms of time, place and person but also has the capability to cater to the needs of health manpower training including medical education. Having been thus based on educational theories, it adopts a scientific approach of learning a complicated skill. The training package takes help of Self Instructional Materials (SIM) and modern communication technology in addition to providing hands-on-training and face-to-face interactions. The distance between a learner and a teacher is a function of dialogue and individualisation. It means if dialogue/academic interaction is possible and the curriculum is need-based, then the effective distance between the learner and teacher is the least. All the training methodologies in distance education systems aim at decreasing this effective distance. The inherent flexibility of the system helps one to learn at one's own pace (slow or rapid learning) and place (minimum displacement from the workplace), utilizes the resources optimally, provides standardised and uniform training, follows objective assessment principles and has the potential to cater to mass education without compromising on quality. Hence, judicious networking and monitoring with an independent appraisal for accreditation could provide an answer to any type of education including medical education. PEDOGOGY OF SURGICAL TRAINING Surgical training is a complex process involving rigorous hands-on training and supervision. In addition, a person needs self-confidence to practise. The whole learning process could be divided into seven steps2 as mentioned below:
Indeed, any complex training could be split into the above seven steps. But the duration at every step of learning will depend upon one's level of past education, experience and the pace of learning. Basic training requires reinforcement and continuity till the skills get converted to long-term memory. In distance education system, the learning continuity and reinforcement is adjusted according to one's own convenience. Though this provides an opportunity for effective learning, a strong component of monitoring at every level needs to be integrated to ensure the actual transaction of this process. Moreover, the provision of mentoring3 at a suitable level could help to ensure quality training. SURGICAL TRAINING-AN ALTERNATE MODEL The main limiting factor for medical education/surgical training has been the cost of infrastructure and equipment. Though sophisticated procedures require sophisticated equipment, most of the life-saving procedures could be performed by time-tested simple techniques. While the performance of sophisticated techniques could be limited to super specialists, simple procedures could be disseminated safely to multi-skilled surgeons to meet the needs of the community. Textbooks and lecture sessions could be replaced by SIM that follows special techniques to meet the needs of adult learners. Viewing operative procedures could be made possible through live transmissions or recorded videos. There is no doubt that a posting in operation theatres is crucial for hands-on-training. The learning process at medical colleges could be restricted to the steps that require the teaching skills of the teachers i.e. demonstrating the procedures while a student assists, and providing learning tips while a student is assisted by the teacher in performing a procedure. The other steps could equally be learnt by a student in any operation theatre (nearer to the residence of the student) where a specialist is available to guide and is also willing to operate to rescue the student during his learning difficulties. In this arrangement, the student has the advantage of learning within the resource constraints, which may be similar to his own set-up in a remote area. This helps in confidence building and one could attempt to perform similar operations in his/her own set-up. Besides, the learning materials available in small set-ups get utilized optimally for training. Thus, not only does the cost of training become affordable but also a large number of doctors could be multi-skilled simultaneously by just involving as many hospitals as necessary. In addition, mandatory residential posting could be avoided for those steps of learning that could equally and effectively be learnt in his own set-up or a in nearby set-up without disrupting his routine activities. Thus, the seven steps of learning surgical skills (as mentioned in the previous section) could be integrated with the distance learning system in the following manner:
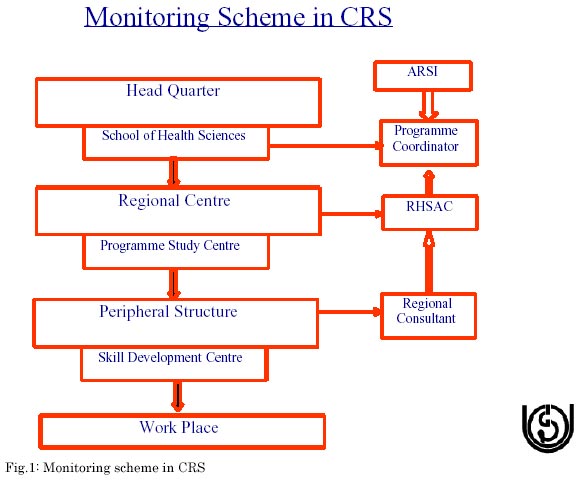
QUALITY ASSURANCE Quality assurance is the hallmark of any training procedure. In the distance education system, due to the involvement of multiple trainers and various procedures, all learning processes are assessed by objective guidelines. There is also an inbuilt mechanism to monitor the whole process through the documentation of every step of learning. Thus, the identification of training institutions and trainers is done as per specific guidelines and logbooks and supervision by counsellors ensures actual performance of planned activities; continuous assessment of students at various levels checks their competency in all major components of learning and the term-end assessment by external examiners provides unbiased decisions. In addition, visits to institutions and periodic meetings of a state-level monitoring committee will add to the quality control mechanism. Independent appraisal by professional bodies, wherever feasible, could give credence to the above system and make the product of such a system acceptable to the law of the land. THE IGNOU EXPERIENCE The one-year programme of Certificate in Rural Surgery (CRS) has been developed by IGNOU in collaboration with the Association of Rural Surgeons of India (ARSI) for postgraduate degree/diploma holders in General surgery/ Orthopaedics/ Obstetrics & Gynaecology. It has been launched in three medical colleges called Programme Study Centres (PSCs) in 2001 and is networked with a few secondary level surgical set-ups called Skill Development Centres (SDCs). The programme package includes a heavy component of practical and actual hands-on-training both at the PSC and the SDC. Besides, it is supplemented with theory blocks, practical manuals, programme guides, assignments, video cassettes, teleconferencing and face-to-face counselling. A maximum of 10 students are selected per PSC based on selection criteria and are posted to the concerned department under an identified senior faculty (counsellor) in rotation so as to ensure that only one student gets posted to any department at any point of time. During the posting the students clear their doubts, assist and perform different operative procedures as planned in the curriculum, maintain logbooks that are counterchecked by counsellors, participate in academic activities of the department and get assessed by the counsellors at the end. A similar pattern of posting and assessment is carried out at the SDCs. The minimum duration of a posting is 45 days at the PSC and 30 days at the SDC spread over one year as per the convenience of the student and the counsellor. At the end of one year, after getting the completion certificate from the PSC and SDC counsellors, a student appears for a term-end practical examination in identified centres having all external examiners, which involves working up of a case, diagnosing spots and also a viva-voce. For the theory component, they have to do 5 assignments-one each in a different discipline and appear in a theory examination which includes 2 papers. Students are required to score at least 50% marks in each of the evaluation components independently. The programme has a three-tier monitoring system-centrally by the programme coordinator, at the state level by the Regional Health Sciences Advisory Committee (RHSAC) that includes the state health officers as members and at a district/peripheral level by a regional consultant. Attempts are being made to widen the professional help from ARSI and other associations. The scheme of the operation of the programme is mentioned diagrammatically. CONCLUSION Distance education can provide quality surgical training that is both affordable and sustainable. The model followed by IGNOU in imparting the Certificate in Rural Surgery (CRS) programme4 has a sound pedagogic basis and can be replicated in developing countries. It also shows that functional integration of all levels of health infrastructure under one umbrella is feasible and self-reliance in health for any nation is possible if the above mode of health training is imparted. Surgeons cutting across different sectors have a key role to play both in imparting the surgical training and monitoring its quality. REFERENCES
Copyright 2003 - Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03010f1.jpg] |
| |||||||||

{kind=link}