 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 65, No. 1, Jan.-Feb. 2003, pp. 55-59 Surgical Training Surgical Training in Africa-A Personal Viewpoint Christine M Evnas Glan Clwyd Hospital, Bodelwyddan, Rhyl, UK
Paper received: June 2002
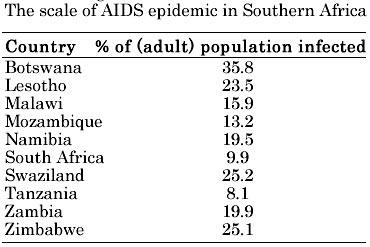
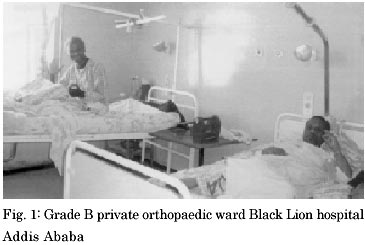
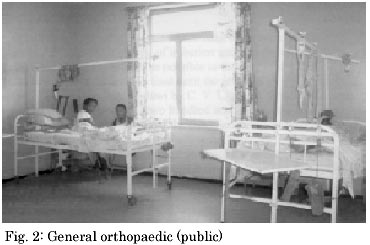
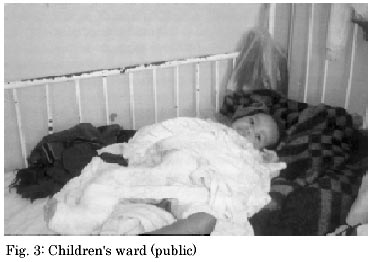
Code Number: is03011 I do not consider myself to be an expert in surgical training in Africa, but I have over the past three years visited eight sub-Saharan African countries and can therefore give you my observations as to what I feel is happening at this moment in time. There are reasons for both pessimism and optimism in Africa about surgery, surgical training and the provision of surgical care. The reasons for pessimism are the increasing problem of HIV/AIDS which is devastating the continent, the lack of money available for provision of services and training, not only in the University Teaching Hospitals more so in the rural areas which are greatly ignored by politicians. Even if the money was ear marked for health care it would appear that due to considerable corruptness in management of healthcare the money doesn't go to where it is actually needed., Included in the bad news (although training is extremely good in most of the University Hospitals which I have attended and these have been five in number ) is that many of the trainees and also medical students and nurses are leaving their countries of training due to extremely poor pay, lack of prospects and the desire to have a better life. On the good side however and therefore these are reasons for optimism. There are many surgeons who still stay in sub-Saharan Africa, who are enthusiastic about teaching, about standards of care, this is both in the public and the private sector which the latter can be used to subsidise the former according to the recent Association of Surgeons of East Africa ASEA meeting which was held in December 2002 in Addis Ababa. The standards of surgical care are being carefully monitored and discussed and there is good and clear insight into what is needed and what is best and what should be done for the future. This was discussed at the ASEA also the development of the College of Surgeons of East Central and Southern Africa (COSECSA) which was launched in 1999, but actually came into being in 2001. The college is enthusiastic about the training of surgeons throughout the Eastern and Southern parts of Africa, they are developing a college which encompasses ten countries. They have now got a financial basis in which to run their college thanks to the generosity of Ethicon at Edinburgh, the Royal College of Surgeons of Edinburgh and the financial backing of the Foundation Fellows who have launched the college. The first examination which will be equivalent to a Membership in Surgery will be first run in December 2003. This will be an exam which will test basic surgical training in orthopaedics, general surgery, including urology and will be aimed at those surgeons who are two to three years into their surgical training. In order to maintain the standards for this examination the hospitals in the whole area will be visited and assessed for suitability for training purposes and the assessment will be done by a combination of local surgical expertise, senior surgeons from neighbouring countries and outside assessor from the United Kingdom with attachments to the Edinburgh College. This is a wonderful new idea and gives great hope for the future of African surgery. Let us take these points a little bit more in detail. First of al HIV / AIDS. This is the scourge of sub-Saharan Africa at the moment. The highest incidence being in Botswana and Zimbabwe. Whether or not this is because these countries test more of their patients, or whether or not it is a genuinely high incidence in that country. I am not sure, but certainly the following table, which was published in 2000, gives an indication of the number of people who are suffering AIDS at the moment. This is a disease which is killing people in their thirties and forties (more than older people) and therefore the countries are loosing many of their highly qualified personnel, this includes, doctors, nurses, teachers, middle management as well as the ordinary labourer and farmer. There was an awful shortage of qualified personnel in hospitals when I visited the Parimyata Teaching hospital Harare in 2002, there were insufficient medical staff to man more than half an intensive care unit, due to loss of doctors from AIDS. There is also a great deal of ignorance concerning HIV amonst health care workers (also hepatitis C). The latter is also important, but doesn't quite make the headlines. Hepatitis C is actually more infective than HIV, but doesn't appear to have the stigma attached to it which the farmer does. For example a female patient in Zimbabwe will not want to know her HIV status because if she informs her husband that she is HIV positive, despite what his status is, she will be divorced. There is at the moment severe paranoia concerning HIV amongst health workers in Sub-Saharan Africa. An extremely excellent paper was presented at the ASEA meeting at Addis Ababa in December given Mercy Nkhalanba for S Mannion from Mzuzu (Malawi). They estimated that twenty to thirty percent of Malawi population was sero positive and they undertook a survey of the attitudes of the Malawi healthcare staff raising awareness of and taking precautions against the occupational transmission of HIV, especially with the operative theatre staff. The initiative consisted of presentations concerning the risks, safe operating theatre practice and what could be done post exposure in view of the lack of anti-retroviral medication. The participants were asked to fill in a questionnaire and two hundred and forty eight health staff (from twenty hospitals in the country) answered the questionnaire. Fifty per ent of them expressed their level of concerns very high, that they were subjected most day to some sort of exposure. Also they felt that if there was exposure that they had a high risk of sero conversion (which is not correct). However, one of the points that was made in the talk is that the incidence of HIV amongst health workers was the same as the normal population and likely to have been acquired through the normal hetero sexual means, but the project did put into practice better availability and increase uptake of protective clothing with better theatre practices. The healthcare workers need to be assured that HIV is not all that easy to catch by handling patients, in fact Hepatitis C is much more likely to be problematic from the point of transmission in health workers as it is more contagious. The HIV safety was brought up also by Rita Peller from Mbarara in Uganda. This was an extremely useful paper concerning the training of surgeons in District Hospitals. Secondly lack of provision of money make the running of all hospitals, both university and other government hospitals out in the districts extremely difficult. The problems in surgery are mainly that of lack of basic essential equipment, in the actual operating theatre itself, for example diathermy. I was talking with a colleague from the University Hospital in Lusaka who told me that there was only one diathermy machine in the operating theatres in the teaching hospital at that moment and that diathermy machine actually belonged to the urologist donated by UROLINK (BAUS) which he had given them a year ago. In order that this equipment survives it is brought to and removed from the theatres at the beginning and the end of each urology list. Also on my visit to The Black Lion Hospital in Addis Ababa, in the theatre suite of six theatres only two diathermy machines were working. I would not consider a diathermy machine a luxury, I would say that for all major open surgery it is absolutely essential, although the surgery can be performed, without diathermy it is much more tedious and much more time consuming. Also endoscopic procedures such as transurethral resection of prostates are impossible without adequate diathermy machines. The other problem with equipment is replacement of parts which become broken and this is especially true of endoscopic equipment which is usually so poorly maintained that it is useless. The situation is not remedied by the fact that often equipment is taken over to these countries, but no provision for replacement is made with the manufacturers which I am sure could or should be provided free from the manufacturer in view of the parlous state of the economies in these countries. This is true of the public sector not the private sector. It also worries me that some of the equipment which is taken over in goodwill by well meaning western visitors, but doesn't see the inside of the government hospital, but is siphoned off to the private sector. If it is used in both I personally have no grumbles, but the provision of equipment should be for the public hospitals. Also the availability of such things as sutures, catheters, double J stents, irrigation fluid is non existent. In Zambia for irrigation in endoscopic procedures in the urinary tract, boiled water in a clean bucket is still the norm, remarkably the patients don't seem to come to too much harm. If equipment is sent from other countries it will also be taxed at the airports due to the money grabbing attitude of the authorities despite the fact that the equipment is usually donated free. If equipment is taken into countries it is best to be carried in, hopefully heavy customs duties can be avoided by negotiation. A paper was given by Rudiger Finger from Germany on "Acceptable Operating Theatre and Surgical Standards in Africa : a continent wide challenge". On visiting several hospitals throughout sub-Saharan Africa he found that among the peripheral hospitals there was not one hospital which had minimal acceptable standards of sterilizing, there was poor composition of instrument sets, no regular maintenance of essential equipment, no one who will take charge of the equipment within the operating theatre, no one to repair the equipment, lack of regular cleaning and disinfectant procedures. This lecture was a massive indictment against the lack luster efficiency of the hospital services, which could be so easily corrected. TRAINING AND SURGERY IN AFRICA On the optimistic side there appears to be a considerable number of projects for improvement of teaching standards in Africa often in conjunction with western countries, Germany features very large in this especially in Uganda and also Canada with its Ptolemy project. This latter is a multi-mode web based e-mail facility available to developing countries from the Unviersity of Toronto it provides it at remarkably little cost and appears to be developing satisfactorily. The surgical training programme in Uganda by the German Foundation of International Development and MBARARA University of Science and Technology has been emphasizing the importance of basic surgical knowledge and train doctors to be able to, after half a year of supervised training to go out into the district to perform operations which might not have otherwise been performed, without supervision especially orthopaedics and general surgery. There is also a Delphi process running in conjunction with the University of Toronto and COSECSA to improve surgical care in East Africa. Also the use of public private mix for alterntive funding is something which should be considered seriously. Five year experience of the Muhimbili Orthopaedic Institute from Tanzania where doctor H. I. Museru pointed out that the East African countries could only meet ten to twenty percent of the required budget for the hospitals with the result that most government hospitals are running at less than twenty-five per cent capacity. In 1996 in Tanzania a law was passed in which public hospitals were allowed to treat private patients. This showed the success of the policy in allowing patients to come into the public hospital and bring in finances with them although there was one considerable problem in this, many of the private patients found that the standards, especially the hospital accommodation were not that adequate, so they needed to be improved. During my visit to the Black Lion Hospital in Addis Ababa I noted that there were two grades of private patients and A and a B grade the A grade getting considerably superior accommodation, but there would appear to be no ethical reason why the public/private mix can't be prevailed upon especially if it is for the benefit of the ordinary man One or two other interesting points which need to be made concerning surgery in Africa is the high rate of infection and it is therefore important that certainly in trauma as little as possible in the way of prosthetic material and internal fixation is used until the problem of sepsis can be overcome. In a paper from Malawi by C. V. Chaheka showed that from October 1996 to October 2002 two hundred and ten internal fixations were performed on various parts of the boney anatomy and twenty six of these patients developed sepsis of which seven were left with serious disability. They pointed out that internal fixation was not widely used due to fear of disastrous results, but that if the infection rate was reduced then the benefits of internal fixation were there to be had, including avoiding a long stay in hospital. COSECSA This is an exciting new venture for The College of Surgeons of East Central and Southern Africa, they are in contact with West African colleagues (who have s separate association). I think that this new departure is going to benefit greatly the standards and enthusiasm of surgeons in the countries involved which include Ethiopia, Malawi, Mozambique, Kenya, Tanzania, Uganda, Zambia, and Zimbabwe at this moment. The membership from this college will allow a generalized standard amongst the countries involved , although at the moment the trainee surgeons undertake university diploma in surgery from their respective universities. This will be a more universal standard with possibly, once the examination has been established and the possibility of a further fellowship examination has been organized, that these qualifications will be interchangeable with the more developed world. It is important however that the examination is tailored to fit the kind of surgery which is performed in Africa especially in relationship to the diseases, for example, tuberculosis and schistosomiasis are common place, trauma is extremely common related to hazardous roads and poor driving. Congential abnormalities also play a major part. Urinary stone disease in the urinary tract below Sudan is uncommon in comparison with Middle Eastern countries and the Far East, but still the management of stones is at least twenty to thirty years out of date. As far as general surgical procedures are concerned I have less information concerning these, but I was interested to note the laparascopic technique were being undertaken with some good success in Kenya and have been undertaken since the early nineties, how they maintain their equipment beats me, but they are obviously managing. However, open surgery at the moment is the mainstay of management of patients in Sub-Saharan Africa. CONCLUSION I have appeared slightly pessimistic in this review, but I would like to point out that I had great satisfaction and pleasure in working in sub-saharan Africa and hope to continue in the future. There is a wonderful welcoming atmosphere in all the countries, the people are keen to exchange ideas and to teach us in the West what they know. Some excellent open surgery is being undertaken. Help with exchange of trainees to the first world is useful, but they need training in the diseases and conditions which they are likely to come across. Increased salaries would improve the number of doctors, especially trained doctors who wish to stay in their country. The drain especially of nurses from Zimbabwe to South Africa and then from South Africa to Europe is unacceptable and we in the west should not be taking nurses who are badly needed in their own countries. Hospitals need equipment, drugs, man power, text books and journals are also useful, but the internet has in fact improved communications dramatically, telephones are worse than useless, postal systems are most unreliable. We have a great need to improve public health education in the town and the countryside in preventing HIV, and venereal disease, but I think there is a generation of young doctors coming up who will in fact improve the situation considerably in these developing countries. Copyright 2003 - Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03011f2.jpg] [is03011t1.jpg] [is03011f3.jpg] [is03011f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}