 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
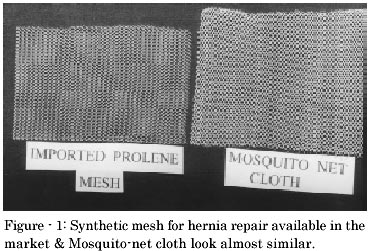
Indian Journal of Surgery, Vol. 65, No. 1, Jan.-Feb. 2003, pp. 89-95 Preliminary Multicentric Trial of Cheap Indigenous Mosquito-Net Cloth for Tension-free Hernia Repair Ravindranath R. Tongaonkar, Brahma V. Reddy, Virendra K. Mehta, Ningthoujam Somorjit Singh, Sanjay Shivade Dr. Tongaonkar Hospital, Dondaicha, Dist-Dhule, Maharashtra-425 408 Paper received: June 2002 Code Number: is03018 Abstract Today world over tension free mesh repair for hernia is the method of choice for adult groin hernia and almost all incisional hernias. Synthetic mesh for hernia repair available in the market is effective, but is very expensive particularly for the poor population in the rural area. It was observed that the ordinary mosquito-net cloth looks and feels quite like a polypropylene mesh and it was thought that its use instead of a standard marketed synthetic mesh could be of significant cost advantage. This net is made of copolymer of polypropylene and polyethylene and can be sterilised by autoclaving. This study analyses the multicentric experience of using the mesh made of the mosquito net since 1996. The preliminary results of 359 hernias in which mosquito-net cloth was used in 4 different centres showed very good results. There was minor infection (stitch abscess) of 4.7%, which healed without a single case of mesh rejection. With follow up ranging from one month to 5 years, there was only one case of recurrence, an incidence of 0.27%. The cost for 7.5 x 15 cm mosquito-net cloth works out to be only 45 paise ( as against Rs.1666/- for the synthetic mesh for hernia repair available in the market), for 15 x 15 cm 90 paise( as against Rs.3724/-), and 30 cm x 30 cm to Rs.3.60 only ( as against Rs.9,430/- ) For economically developing country like India, use of this cloth for repair of hernias is strongly recommended. Key Words: Hernia, Mesh repair, Hernioplasty, Cheap Material, Mosquito-Net Cloth INTRODUCTION Operations for hernia is the commonest surgical procedure performed.1 Majority of the groin hernias in adults need some kind of repair of the weakness in the posterior wall. Bassini's repair modified by Shouldice undoubtedly proved very good with very low recurrence rate of only 0.8 %, if done by dedicated senior surgeons but in the hands of general surgical community the results were much less satisfactory.2 The recurrences varied form 5.9 to 6.5 %.3 Berliner's modification of Shouldice's using 2 layers of repair, though simple, surgeons in training find the method difficult to master and so produce poorer results than their senior colleagues. Moreover in these methods there is undue tension on the suture line and in addition there is histological and biochemical evidence that inguinal hernia can be caused by a metabolic disorder involving collagen turnover of the transversalis fascia, therefore utilisation of this already defective tissue in the repair of hernias is counter-productive, while replacement by synthetic material seems a more logical approach. 3, 4 Therefore in last few years there is an impressive rise in the popularity of the Tension Free Hernioplasty using prosthetic mesh popularised by Liechtenstein and Schulman and today world over it is the method of choice. Mesh repair of hernia is simple to perform, gives excellent results with recurrence rate of 0% to 0.2 %, low complications rates and early return to full activity, at the same time for surgeons in training it is easier to master than Berliner or Shouldice repair. 2, 3 The question is which mesh to use. It is undoubtedly has to be made of non-absorbable material. Many types of meshes have been tried like stainless steel mesh, polyester cloth, nylon cloth, dacron mesh, teflon mesh and marlex mesh.. Pioneered by Francis Usher, in 1958 the first generation of marlex mesh was made of polyethylene. It was good but polyethylene was difficult to sterilise because of its low melting point. Therefore in 1962 polypropylene was developed, which satisfies all the requirements of an ideal mesh and therefore 'Prolene Mesh' today is the best material available. 4, 5 But the imported 'Prolene Mesh' available in surgical shop is very costly. A 7.5 x 15 cm mesh costs Rs. 1,666/- while a 15 cm x 15 cm mesh costs Rs. 3,724/- and for big incisional hernias the cost it is much more, 30 cm x 30 cm costs Rs.9,430/-. This cost is very much prohibitive for our poor rural patients. Therefore many Rural Surgeons were in search of cheaper material. In 1996 one of the co-authors found out a good mosquito-net cloth, which was very similar to the synthetic mesh for hernia repair available in the market (Figure-1) and started using it for hernia repairs with excellent results. Manufactured by Banglore Mono Filaments Pvt, Ltd. from Bangalore, this cloth was found to be much cheaper than the polypropylene mesh, about Rs.40 for a meter. When cut into pieces, The cost of cloth for 7.5 x 15 cm works out to be 45 paise, that for 15 x 15 cm 90 paise and for 30 x 30 cm Rs.3.60 only. Since it was introduced to the principal author he started promoting it and introduced it to many surgeons who have started using the cloth with encouraging results. Hence this study was carried out with the following aims and objectives: 1) To study the properties of this cloth as regards its composition,
its suitability
for sterilisation by autoclaving and tensile strength
MATERIAL AND METHODS To find out the composition and other properties of the Mosquito net, the piece of cloth was sent to a renowned research institution approved by Govt. of India ARAI (The Automotive Research Association of India) based at Pune and results were obtained. The manufacturer was contacted and details of the cloth obtained. The clinical trials were carried out at four different centres. The basic theme of the clinical trial was to study the effect of use of indigenous cheap mosquito net cloth as mesh for repair of various hernias in the patients. As the trials are conducted independently, the details varied from centre to centre and are given in Table-1 & Table-2. The method used by the principal author in centre I is given in details and the main variations of methods used at other three centres are mentioned. Clinical Trial In Centre I: Period of trial was from 10th April 2000 to 10th Feb.2002 (22 Months) There were total 124 patients who underwent hernia surgery out of them 23 were small children on whom only herniotomy was done, 29 underwent herniorrhaphies or anatomical repairs, while in 72, mesh was used. There were 7 bilateral cases so total meshes used were 79. out of which 63 were inguinal, 4 were incisional and 12 were other hernias. Prolene mesh was used in 2 cases and in all other 77 cases mosquito net cloth was used. In one patient with bilateral inguinal hernia on one side mosquito-net cloth and on other side prolene mesh was used so that the patient himself could act as 'Control' for this study. The age group varied from 30 to 85. There were 2 recurrent hernias, 2 strangulated and one sliding hernia in the series. All surgeries were done by the author himself. a) First the cloth sent by the co-author for trial was given trial of double autoclaving putting the piece of mosquito cloth in a paper envelop along with signaloc to verify proper sterilisation by autoclaving and effect of autoclaving on the quality of the cloth was observed. b) Informed consent from the patient and relatives were taken showing them both, a piece of synthetic mesh for hernia repair available in the market and the mosquito net cloth and only if they agreed to the use of the mosquito net, it was used for repair. No additional charges were taken for the mosquito-net cloth. c) Whether to do repair using mesh or to do herniotomy or herniorrhaphy was decided on the operation table. Steps of operation Groin Hernias Prolene 1-0 suture was used to fix meshes in all cases. The method used to fix the mesh was similar to that described by Liechtenstin6 except following modifications.
Incisional (Ventral) Hernias and Other Hernias: Procedure was similar to that used for onlay repair using any other mesh, with following modifications.
Routine antibiotic were used in all cases where mesh was used. Post operative complications related to use of mesh like infection, seroma formation, pain, rejection or recurrence etc. were noted during the hospital stay and later till the patient had any complaints. Follow up All the patients were called for follow up upto 1 month and were instructed to report further if there was any complaint regarding hernia operation. Clinical Trial in Centre II This is the original rural centre in Andhra Pradesh where the use of this cloth was started by the co-author in 1996. All surgeries were done by the co-author himself. Clinical trial period was from 5-7-1996 to 27-6-2001 (5 years). In this period total 198 mesh repairs were done, out of them mosquito-net cloth was used in 157 cases, marlex mesh in 16 and prolene mesh in 25. Suture material used for fixing the mesh was either nylon strands or sutupack (monofilament polyamide). Out of 198 cases, 99 were inguinal hernias, 95 were incisional hernias and 4 were other hernias. He also studied the tensile strength of the mesh by using hooks and weights in different rows of three types of meshes. Clinical Trial in Centre III This is an institutional trial done in a rural medical college. Surgeries were done by 4 persons including trainee residents. Mesh repair was done in 94 patients out of which prolene mesh in 11 patients and mosquito net in 83 patients. (7 were bilateral) thus total 101 meshes were used. 80 patients had inguinal hernia, 9 had incisional hernia and 5 had others hernias. Different suture materials were used to fix the mesh. Out of 94 cases chromic cat gut was used in 21 cases, while silk was used in 58 and prolene was used in only 15 cases as suture material. After autoclaving the mesh was preserved in Cidex. Clinical Trial in Centre IV This is another rural centre run by a rural surgeon who did the trial since November 2000 to Jan 2002. In this period total 52 patients underwent hernia surgery out of which 39 were treated using mesh. There were two patients with bilateral hernia thus total 41 meshes were used. Out of which prolene mesh was used in 6 and in remaining 35 mosquito-net cloth was used. There were 29 inguinal hernias, 7 incisional hernias and 5 other hernias. In all cases prolene was used to suture the meshes. RESULTS Composition and other properties of the mosquito-net cloth 1. Report from ARAI [personal communication- letter dated 6-9-2000 Ref. No MTL/200008/NK/CM/1236OCNo.1236] the observations are- a) Material under test is copolymer. It is
poly (Ethylene-co-propylene).
2. Report from the manufacturer Bangalore Mono Filaments Pvt Ltd., [Personal communication, letter dated 23-3-3001 Ref. No. BMF/BNG/882/2000-2001] a) The fabric is made out of high density polyethylone. (Please note-it is ethylone
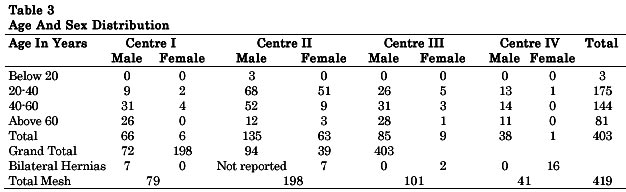
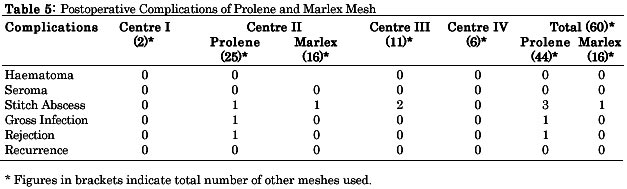
& not ethylene) 3. Study of tensile strength done in centre II showed clearly that the tensile strength of mosquito-net was almost equal to that of marlex mesh but slightly inferior to prolene Clinical Trial In all study included 403 patients on whom total 419 meshes were used. Age varied from 18 to 85 years. The common age group was between 20 to 60 [Total 319 out of 403]. There were 324 males & 79 females. In groin hernia group there was only one woman. Rest all other women had either incisional hernias or other hernias. [Table 3] Out of total 419 mesh repairs for hernia in 359 cases mosquito-net cloth was used. There was not a single case of rejection and all cases healed well. On the contrary out of 44 cases in which prolene was used there was one case of rejection due to persistent severe infection. (Tables 4 & 5). In Mosquito-net series there was only one case of gross infection which was not because of mesh itself but because it was a case of huge infected incisional hernia with ulcer (Figure-3) and contamination of wound due to opening of bowel and postoperative sloughing of skin edges probably due to extensive dissection. Wound healed after 2 months by secondary intention. There is no rejection. (Figure 4). Minor stich abscesses which healed subsequently were seen in 17 cases (4.7%) out of 359 meshes. This incidence was less as compared to combined prolene and marlex mesh, which was 4 out of 60 (6.66%). Haematoma formation in 3 cases was reported only by one centre. They were cases of big inguino-scrotal hernias, which needed extensive dissection. Seroma formation was found in 3 cases- all were incisional hernia cases. One case in centre IV needed repeated aspirations. Out of 359 cases of mosquito-net there was only 1 case of recurrence (0.27%). This case was operated by junior- most resident in the teaching institution. DISCUSSION The use of Prolene mesh for repair of Hernias is an already established fact4,5. The only factor for our poor patients is the cost. The Mosquito-net cloth used in this trial appears to be cheap and perfect substitute for the costly synthetic mesh for hernia repair available in the market. Safety & other properties of the cloth The Prolene mesh is made of polypropylene. The mosquito-net cloth is Copolymer of polyethylene & polypropylene. The use of both latter materials individually has been well established in clinical practice since 1958 & they are found to be safe. The mosquito-net cloth belongs to the same category of material, so naturally has the same properties, strength and inertness required of a suitable biomaterial. In the clinical trial period ranging upto 5 years the cloth has not shown any adverse effects so far. Suitability for sterilisation by autoclaving The mosquito-net cloth is sterilised by autoclaving. Steam sterilisation by autoclaving is the safest & surest method of sterilisation 7. The melting peak temperature of the material used is found to be 144-59°C (for polyethylene it is 110-130°C while for polypropylene it is 155-165°C). In any type of autoclave the temperature does not go above 132°C. In gravity displacement type of autoclave it goes upto 121-123°C. While in High speed pressure steriliser or pre-vacuum steriliser it goes upto 132°C7. Therefore the mosquito-net cloth can be easily sterilised by any method of autoclaving which guarantees its sterilisation. The cloth is made of monofilament fibres, so unlike multi-filament and braided materials it is less likely or unlikely to harbour bacteria, therefore there is hardly any chance of infection due to the mosquito-net mesh itself4. The incidence of infection and rejection in monofilament meshes is very little. In Liechtenstein series the infection rate was 0.03% & rejection of mesh was 0% 3 . In present trial also there was not a single case of rejection (0%) and only minor stich abscesses in 4.7% There was only one case of gross infection (0.27%) which was not due to mesh & even in presence of infection the mesh was not rejected and the wound healed subsequently. The recurrence in one case (0.27%)in the series was probably because of technical error. The operation was done by the junior most trainee resident in the teaching institution which was later corrected by putting an additional mesh. In the hands of experienced individual surgeons there was not a single case of recurrence. The common cause of recurrence according to Lichtenstin group is technical errors involving inadequate overlap of mesh on the pubic bone and placement of mesh under tension. If these are taken care of the recurrence will be negligible3. CONCLUSION Indigenous mosquito-net cloth has properties similar to synthetic mesh available in the market and can be safely used for hernioplasty by mesh repair. Its works out to be 3700 times cheaper. REFERENCES
Copyright 2003 - Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03018t5.jpg] [is03018t3.jpg] [is03018f4.jpg] [is03018f2.jpg] [is03018t4.jpg] [is03018f1.jpg] [is03018f3.jpg] [is03018t1.jpg] [is03018t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}