 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
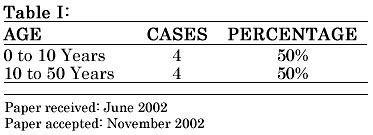
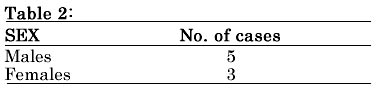
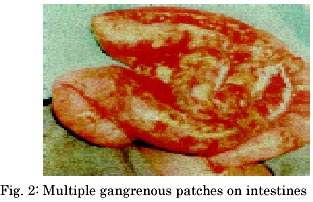
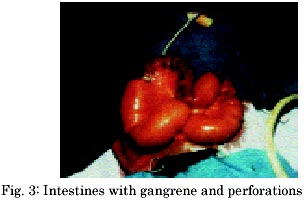
Indian Journal of Surgery, Vol. 65, No. 1, Jan.-Feb. 2003, pp. 96-98 Surgery for Necrotising Enteritis in a Rural Hospital K. Dakshinamoorthy Nagai Hospitals, 3/134 Main Road, Puthur, Nagapattinam-611 106 Paper received: June 2002 Code Number: is03019 Abstract Necrotising Enteritis is an inflammatory disease caused by a virus. The onset, progress and fatal end occur rapidly in succession, and a quick decision on the surgical treatment is necessary. Resection and end to end anastomosis is useful. Key words: Necrotising Enteritis, resection and end to end anastomosis. INTRODUCTION Necrotising enteritis is an epidemic, especially between May-July in the area of the author's practice. The onset, progress and the fatal end are in quick succession-within 48 hours. A quick decision on the surgical line of treatment is therefore essential to save the life of the patient. MATERIAL AND METHODS Nagapattinam is a coastal rural town in the state of Tamil Nadu. It has got a district headquarters hospital which caters to a population of about 80,000. The main aim of this paper is to present our experience in the surgery on Necrotising Enteritis and to evolve a surgical procedure for the treatment. The study was carried out over a period of 2 years. During this period 72 cases of Intestinal obstructions were subjected to Laparotomy, out of which, 8 cases (11 %) turned out to be of Necrotising enteritis. Four (50%) cases belonged to the age group between 0-10 years and the remaining 4 (50%) belonged to a broad age group between 10-50 Years. The youngest was a 3-year-old male boy and the oldest was a 48-year-old male adult. The male to female sex ratio was 5:3. All these cases were admitted with a similar clinical presentation of pain over the abdomen of 12-24 hours duration. Almost all cases also presented with vomiting. Their general condition was very poor with severe dehydration and toxaemia. The abdominal examination revealed generalised distension and tenderness all over the abdomen with a rigid abdominal wall. 50% of the cases revealed a palpable vague tender mass either over right or left iliac fossa. There is no specific diagnostic test available for necrotising enteritis and the radiological findings vary from case to case. However 4 (50%) cases revealed typically multiple fluid levels of obstruction. One case presented with single fluid level and another case showed distended loops of small intestines. One case showed a large colonic shadow and yet another showed a diffuse opacity inside the peritoneal cavity. In this series, the pathology of Necrotising enteritis was noticed mostly in the ileum (75%) whereas jejunum was involved in 25% cases; the colon was not affected in our series. The length of the involved intestine was usually 2 feet to 5 feet. Based on the naked eye appearance of the intestines, the necrotising enteritis can be classified into 3 stages. Stage I: 0-12 hours: Intestines are rigid, inflammed, spastic, pipe -like and oledematous (Fig:1) Stage II: 12-24 hours: Intestines are that of Stage I accompanied by multiple gangrenous patches (Fig.2). Stage III: 24-48 hours: Intestines are that of Stage II and have multiple perforations. This stage is otherwise known as stage of gross peritonitis and it is very difficult to save the patient at this stage (Fig.3). A quick decision on the surgical line of treatment has to be taken, lest the patient will die of toxaemia. "Resection and end to end anastomosis" is the treatment of choice apart from peritoneal toilet, which was carried out in all the 8 cases. The histopathological examination of the resected specimen revealed inflammatory and haemorrhagic areas with increased vascularity and sinus histiocystosis. RESULTS With the limited number of antibiotics available in rural sectors, an immediate operative line of treatment of resection and anastomosis without loss of time, is the only choice of treatment left and the result appears to be very rewarding. All the seven patients who were operated within 24 hours of onset of pain over the abdomen recovered fully. But only one 3-year-old male baby died during the postoperative period due to aspiration pneumonitis. DISCUSSION The main aim of this study is to present the experiences on the "surgery on necrotising enteritis" and to evolve a surgical procedure for the treatment. The causes of intestinal obstruction due to inflammatory diseases are very few. There is no pre-operative, specific diagnostic test for necrotising enteritis. It is very difficult to diagnose necrotising enteritis clinically as well. Hence, it is always a per operative diagnosis in the rural sectors. The main problem in the rural area is that the patients are brought to the surgeon in stage III (i.e with gross peritonitis and with severe dehydration and toxaemia.) Most of the patients cannot afford the 3rd generation antibiotics and hence one has to treat the patient with 2nd generation antibiotics. For blood we have to depend on "Direct Blood Transfusion" (blood collected from relatives, tested and cross-matched with the recipient's blood and transfused) since the licenced blood banks are quite far away. Another interesting feature in the present series is that only the jejunum and ileum were affected and colon was not at all affected. In other words the infection never crossed the ileo caecal barrier. The cause of necrotising enteritis is a virus. In the author's area, most of the people are fish eaters. One particular type of fish called "Flying fish" is available during months of May to July; whether this kind of fish is a carrier of the virus is not known. Copyright 2003 - Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03019t1.jpg] [is03019f2.jpg] [is03019f1.jpg] [is03019t2.jpg] [is03019f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}