 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
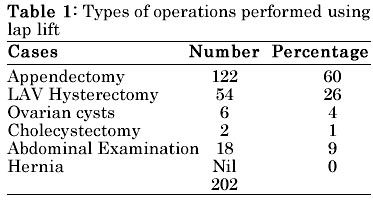
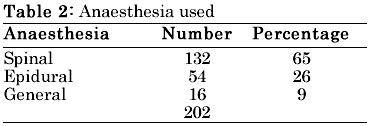
Indian Journal of Surgery, Vol. 65, No. 1, Jan.-Feb. 2003, pp. 99-101 Cost-effective and Gasless Laparoscopic Surgery for Rural Hospitals K. Dakshinamoorthy Nagai Hospitals, 3/134 Main Road, Puthur, Nagapattinam-611 106. Paper received: July 2002 Code Number: is03020 Abstract Lift laparoscopy is ideal for rural hospitals because it is cost-effective. This procedure, which avoids using gas, prevents many complications that are encountered in laparoscopy done with gas. Key words: Laparo-lift, cost-effective, gasless, laparoscopy INTRODUCTION We have witnessed many developments in surgical procedures in the last decade. Laparoscopic (Mini-hole or Minimal invasive) surgery is the latest amongst these. Even though every surgeon is very impressed and attracted by this latest technology, he is unable to give the benefits of this technology to his patients due to the high cost involved in purchasing instruments for this procedure. Therefore the author has adopted an inexpensive, simple 'Laparo-lift' (Gasless) laparoscopic technique. MATERIAL AND METHODS The aim of this paper is to present the author's experiences of an inexpensive laparoscopic procedure without recourse to using gas and thereby inducing more rural surgeons to use this technique. The period of the study is three years, from January 1999 to December 2001. 202 patients were subjected to Lift Laparoscopy for various operations as listed in Table 1 during this period. The series includes only two cases of cholecystectomy as the area of the author's practice has a low incidence of calculus cholecystitis. For lack of confidence, the author has avoided performing laparoscopic hernia repair. Only 8 cases belonged to the age group of 12-15 years, the rest of the cases belonged to the age group of 16-86 years. THE ECONOMICS Instruments: The author has purchased telescope, camera, hand instruments and a Laparo-Lift set from different companies for less than 2.5 lac rupees (Fig. 1) and this includes the instruments trolley (Fig. 2). Not purchasing the air and carbon dioxide insufflators reduced the overall expenditure by almost 25%. Anaesthesia: All appendectomies were done under spinal anaesthesia and all lap-assisted vaginal hysterectomies were performed under epidural anaesthesia. General anaesthesia was administered to patients by their choice and was also used for children below 15 years (Table 2). Air and carbon dioxide insufflation were not used and instead a mechanical Laparo-Lift was used to lift the abdominal wall. The technique of Laparo-Lift involves the use of two blades of 0.2 cm thickness (1"width x 3"length) inserted into the peritoneal cavity through the 1.5 cm infra- umbilical main port. The blades are then widened inside the abdomen forming an angle between them. A vertical rod is then fixed to the handle of the blades and the other end of the rod can be aligned and screwed to a higher horizontal bar, which is also fixed to the side of the operation table with a second vertical rod (Fig.3). A 10 mm trocar is inserted into the abdomen through the main infra-umbilical port under the Laparo-Lift blades. The telescope with the camera is inserted through the 10 mm trocar. By this technique there is enough free intra-peritoneal space for any laparoscopic manipulation. There is no increase in the intra-abdominal pressure which is an unavoidable feature in laparoscopy using gas. The other ports can be placed according to the convenience of the operating surgeon. It might be noted that, perhaps, conversion for one trained in laparoscopy with gas to lift-laparoscopy might be difficult. The converse is not true. Advantages: There are several advantages of Lift-laparoscopy in contrast to laparoscopy using gas.
Failures The author failed in his first four cases and had to convert them into open surgery since he did not want to tax or strain his team for more than four hours. Failures occurred because of
This, however, had nothing to do with the procedure being gasless. In open surgery, the eyes and hands work in the same field whereas in laparoscopic surgery the eyes and hands must work in different axes. Surgeons should have a good general surgical grounding, patience to learn and adapt and also the ability to invest money in order to graduate to becoming a laparoscopic surgeon. RESULTS One patient died on the table of disseminated intravascular clotting (D.I.C.), a rare complication, difficult to manage in the best of circumstances. Two cases developed incisional hernia at the main infra-umbilical port and were subsequently repaired. One case suffered injury to the urinary bladder (1.5 cm) while separating the bladder from the cervix and the rent was closed in layers by intra-corporal knotting. Two cases developed surgical emphysema, which subsided within twenty-four hours without treatment. DISCUSSION Initially, the author was hesitant to adopt this technique on two counts: 1. Apprehension about the ability to learn the technique and 2. Considerations of monetary returns. Rural surgeons are taking recourse to Lift-laparoscopy in the interests of the patient, for example, less postoperative pain, shortened hospital stay, and consequently, early return to work. CONCLUSION Lift-laparoscopy is likely to benefit the rural patient. It is effective and economically more practical. Copyright 2003 - Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03020f3.jpg] [is03020t1.jpg] [is03020f1.jpg] [is03020f2.jpg] [is03020t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}