 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 65, No. 2, March-April, 2003, pp. 163-167 Tension-free open mesh plug repair versus Shouldice repair under local anaesthesia in groin hernia Bholla Singh Sidhu, Ranpinder Kaur Sidhu Department of Surgery, Unit I, Govt. Medical College and Guru Nanak Dev Hospital, Amritsar, Punjab.
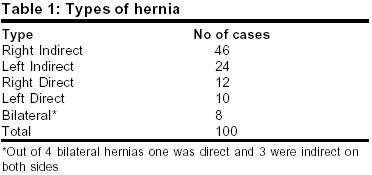
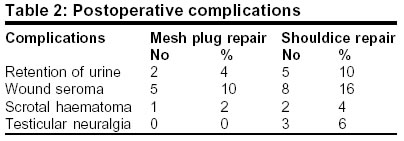
Paper Received: February 2002, Paper Accepted: November 2002. Source of Support: Nil Code Number: is03028 ABSTRACT Since the mid 1980s, dramatic progress has been made in the surgical treatment of hernia in respect of the use of prosthetic mesh. Results in 50 cases of primary groin hernia treated by mesh plug repair were compared with those in a similar number undergoing Shouldice repair under local anaesthesia. The mesh plug repair appears to be an easy, simple, efficient and quick procedure, which can be employed to repair virtually any type of primary or recurrent groin hernia. It is associated with less operative morbidity and less short-term and long-term postoperative discomfort. The study has also confirmed the safety, efficacy and convenience of using local anaesthesia which is `patient-friendly' and cost-effective and allows an early discharge of the patient. Our experience shows that it can be learnt easily and quickly and should be used as a routine procedure for all groin hernias requiring reinforcement. KEY WORDS: Hernia, groin, Mesh repair, Plug repair, Shouldice repair How to cite this article: Sidhu BS. Sidhu RK. Tension-free open mesh plug repair versus Shouldice repair under local anaesthesia in groin hernia. Indian J Surg 2003;65:163-7. INTRODUCTION Ambulatory surgery for hernia has become the need of the hour. Since the mid 1980s there has been an increase in the use of prosthetic mesh in surgery for hernia. Rutkow1 had predicted that out of 7,50,00 hernia operations performed in the US in 1998, almost 80% would involve the use of mesh prosthesis. The tissue-based groin herniorrhaphy techniques create tension on the suture line, are difficult repairs to perform, and are associated with greater number of complications. Also, the level of patient discomfort and disability is higher coupled with prolonged convalescence. The failure rate for the repair of primary groin hernia using the patient's own tissues is unacceptably high, approaching 15%, with an even higher percentage for the repair of recurrent hernia.2 Usher3 was the first to report the use of prosthetic polypropylene mesh in the repair of inguinal and incisional hernia. Lichtenstein4 began using a rolled or cylindrical or cigarette mesh plug for treatment of femoral and recurrent inguinal hernia and reported its efficacy in 1974. Gilbert5 in the late 1980s improved upon the Lichtenstein device by fashioning a flat piece of mesh into a cone or umbrella. Learning of his success with this technique, Rutkow and Robbins6 began using hand-fashioned umbrella plugs in 1989. By the end of 1991 they were using mesh plugs to treat all types of inguinal hernia7. Since 1993 they have started using pre-manufactured umbrella `Marlex mesh' and found it simpler to use than a hand -fashioned plug. In 2400 mesh plug repairs, they have reported a recurrence rate of less than 1% in primary hernia and 2% for recurrent hernia. Fisher et al9 in their phase II evaluation of the Marlex plug in an unselected cohort of 72 patients of groin hernia in 1997-98, found the results comparable to or even better than those after laparoscopic and Shouldice repair (SR) respectively. SR is considered the current golden standard for herniorrhaphy with a recurrence rate of 0.2%. However, the results are not always reproducible in non-specialist centers. The tension created in the repair accounts for a prolonged period of postoperative pain and abstinence from normal activities and work for at least 6-8 weeks. The mesh plug repair (MPR) is a tension-free repair adaptable to any groin hernia, including recurrent hernia. It offers excellent patient comfort and satisfaction, a short hospital stay, rapid rehabilitation and lower complication and recurrence rates. MATERIAL AND METHODS We have evaluated the mesh plug tension-free technique in 50 cases of type 2-5 primary inguinal hernia,10 in relation to postoperative hospital stay, pattern of various postoperative complications and convalescence. The results have been compared with those of Shouldice repair performed in another group of 50 cases. The patients were randomized to enter either group. The age of patients ranged from 21-90 yrs, with a mean of 53.8 yrs. 46 patients led sedentary lifestyles and 54 were involved in strenuous work. 58 hernias were right-sided, 34 left-sided and 8 were bilateral primary inguinal hernias. Out of 76 indirect hernias 16 were of Gilbert-Nyhus type 2, 50 of type 3 and 10 of type 4. Out of 24 direct hernias 16 were of type 5 and 8 of type 6 (Table 1). MPR was performed in 36 indirect and 14 direct hernias and SR was done in 40 indirect and 10 direct hernias. OPERATIVE TECHNIQUE All patients were operated upon under local analgesia supplemented with intravenous sedation with diazepam and pentazocine whenever necessary. All patients received a single intravenous dose of Inj. Ceftriaxone 1 gm before starting the operation. The local anaesthetic mixture (LAM) of 1% lignocaine and 0.5% bupivacaine with 2-3 ml of 7.5% sodium bicarbonate solution was used by layer-wise infiltration technique. 8 to 10 ml of the solution was injected beneath the external oblique aponeurosis (EOA) to flood the inguinal canal to anaesthetize all three nerves in the region. A 4-6 cm transverse incision was made over the region of the deep inguinal ring. After flooding the canal with the LAM, it was opened to expose the structures. The ilioinguinal and genitofemoral nerves were preserved. The cord was mobilized, the cremasteric fibres were split and the indirect hernia sac was dissected free of the cord structures high up to the extraperitoneal fat pad. The sac was not routinely opened but was simply inverted into the internal ring. A complete scrotal hernia sac was divided at its middle and the proximal part is inverted into the internal ring. Since the pre-manufactured mesh plug was not available and is very expensive, a hand- fashioned polypropylene mesh plug, made from a 7.5x7.5 piece of the mesh, was inserted tapered end first into the internal ring and pushed beneath its crurae. The plug was kept in place by inserting 4-6 interrupted 3/0 polyglactin sutures through the outer margins of the plug and the crurae. These are not strength sutures but only holding sutures to keep the plug in position, and any crural tissue, even if flimsy suffices. In direct hernia the attenuated fascia transversals is incised near the base all around to create an extraperitoneal pocket which accommodates the plug after the sac is introflected. The plug is held in place by interrupted sutures. All indirect and direct MPRs are further reinforced by a second piece of flat mesh 9 cm x 6 cm. The onlay patch is placed by a sutureless technique on the anterior surface of the posterior wall of the canal from the pubic tubercle to well above and lateral to the internal ring. The lateral portion of the pre-shaped onlay patch was split to allow the passage of the cord. The split was sutured on itself to provide an opening for the cord while functioning as a pseudo internal ring. The onlay patch is not an integral part of the repair but is intended solely to strengthen the direct space, thus serving as prophylaxis against future direct herniation by creating further tissue growth in the remaining part of the wall. In case of direct hernia the patch shall prevent any future indirect herniation. A loosely running 3/0-polyglactin suture was used to close the EOA. The Scarpa fascia and the subcutaneous tissue were approximated by interrupted chromic 3/0 catgut, and the skin by interrupted 3/0 polyamide suture. A self-adhesive transparent dressing (Tegaderm-3MR) was applied over the sutured wound. Patients were discharged from the hospital as soon as possible with a prescription to take tab. Acetaminophen 650 mg., Propoxyphene napsylate 40 mg, and Ciprofloxacin 750 mg twice daily for five days. All patients were motivated to be ambulatory from the evening of the operation and to resume normal activities as soon as possible. 50 cases of inguinal hernia were operated under local anaesthesia using Shouldice technique as described by Glassow.11 During all MPRs the mesh was routinely soaked in an antibiotic solution prepared from 80-mg tobramycin in 500 ml of normal saline to prevent any bacterial adherence to the mesh. The assisting nurse was instructed to spray a jet of the antibiotic solution on the wound margins and the surrounding skin every 5-10 minutes alternating with a similar spray of the LAM into the wound. The LAM and the antibiotic solution were sprayed into the wound during SRs also. RESULTS The hospital stay in MPR ranged from 0-2 days with a mean of 14 hrs. In SR the hospital stay ranged from 0-7 days with a mean of 2.5 days. No patient required readmission to the hospital. The operating time for MPR ranged from 35-50 minutes, with a mean of 37 minutes. The range for SR was 35-60 minutes, with a mean of 56 minutes. Patients in both the groups were given intramuscular diclofenac sodium in the immediate postoperative period, none of the patients in MPR group complained of any wound pain or testicular neuralgia. All patients were discharged with a prescription of propoxyphene napsylate and acetaminophen combination for a week; all patients remained free of pain. On the same analgesic schedule 4 patients in the SR group complained of severe testicular neuralgia. These 4 required tramadol parenterally for effective relief of pain. 2 of these required an oral schedule of analgesia for a two-week period. In the MPR group 4% had postoperative urinary retention as compared to 10% in the SR group. The incidence of wound seroma in MPR and SR was 10% and 16% respectively. Scrotal haematoma was observed in 2% and 4% respectively. It resolved on conservative treatment in all but one case and that required aspiration. 6% cases in the SR group complained of testicular pain as compared to nil in the MPR group (Table 2). In a short follow-up of 95% cases for 25 months with a mean follow-up of 18.5 months, there was no recurrence. The mesh was not rejected in any of the cases. DISCUSSION In the present study of MPR, a hand-fashioned polypropylene plug was inserted into the hernia defect and was kept in position by multiple interrupted sutures. An onlay patch further reinforced the repair by sutureless technique, placing the patch on the anterior surface of the posterior wall of the inguinal canal. While comparing the results of MPR with those of SR, it was observed that MPR took on an average 35-37 minutes, whereas SR took 55 minutes. Overall, MPR was associated with lesser postoperative complications than SR. In no case was there any need to remove the mesh. The average hospital stay in the case of MPR was 14 hours, whereas in SR it was more than 2 days. Thus, MPR has advantages of early ambulation and early return to work with better patient compliance. In a short follow-up of 25 months no recurrence was observed in either group. Pain and discomfort were significantly less in the patch and plug repair. Nashimura et al,12 while comparing the MPR technique for adult inguinal hernia with conventional sutured repairs, concluded that MPR for adult inguinal hernia is a useful operative procedure with a shorter operating time, less postoperative wound pain and almost the same recurrence rate as seen in conventional repairs. They also proved that there is no significant difference in the postoperative white cell count and the CRP between patients with conventional sutured repairs and MPR. In Robbin and Rutkow's 8 experience of treating more than 6000 patients of hernia and more than a decade of experience with the mesh plug, it was observed that the use of MPR under ultra short-acting epidural anaesthesia, essentially eliminated postoperative urinary retention. They did not observe any correlation of pain and numbness with the preservation or sacrifice of ilioinguinal and genitofemoral nerves. They recommend several months of conservative treatment for all cases of ilioinguinal and genitofemoral neuralgia following groin hernia surgery. None of their patients required repeat surgery for this condition. They have opined that it is the tension-producing repair, not the rare entrapment of a nerve, which is the cause of pain. Dieudonne,13 in a recent publication on plug repair of groin hernias has published results of 3332 plugs inserted in groin hernias. On a ten-year follow-up there was a 1.4% recurrence rate. They used only plugs and no onlay patches. They observed no significant difference in chronic postoperative pain between prosthetic and Shouldice surgery. The risk of plug shrinkage and migration appears to be exceptional and rather minor considering the thousands of operations performed. In their Shouldice surgery, pain was attributed to the use of steel threads in the repair. After a 10-year experience with plug repair they have abandoned Shouldice repair. The mesh plug hernioplasty is a technically simple surgical operation, which, in a standardized form can be used to repair any groin hernia thus obviating the need for differing repairs for various types of primary and recurrent hernias. The secret is to master the technique. There is paucity of reports in the literature with regard to umbrella plugs eroding into nearby structures or of unsuspected migration. Similarly, no scientific documentation of umbrella plug shrinkage leading to recurrence is available. Most impressively, the umbrella plug hernioplasty helps reduce postoperative morbidity and short-term and long-term discomfort. The repair entails much less dissection and traumatization. Most surgeons do not routinely open the hernia sac for manual or visual inspection. In all reducible hernias it is best that the unopened sac be placed back into the abdominal cavity, the inverted hernia sac involutes in a few days without any problems. Ligation of the sac at its neck, a routine practice till recently, produces a miniature peritonitis contributing to postoperative discomfort and malaise. MPR in multirercurrent hernias had a recurrence rate of 9%. In the Robbin and Rutkow series 8, they suggest an alternative approach for such hernias, including an anterior preperitoneal approach, Nyhus repair, an anterior preperitoneal giant prosthetic reinforcement of the visceral sac (Stoppa and Wantz) or a posterior preperitoneal laparoscopic repair. An extensive international experience in the repair of virtually all groin hernias with a mesh plug has resulted in a low recurrence rate combined with a marked diminution of postoperative complications. The mesh plug repair does not require expensive and technologically advanced equipment. It is also among the easiest of hernia repairs for the average surgeon to learn and has a minimal learning curve. The technique concurs with the present growing advocacy of surgical minimalism. On the other hand, SR is difficult to perform in obese patients and in those with thin and stretched fascia transversals. It is not an easy technique to learn as confirmed by the practice at the Shouldice Clinic, where 100 operations need to be done by the staff as assistants before embarking on their own. A major contribution made by the Shouldice Clinic was the demonstration of the value and efficacy of local anaesthesia14. The safety and efficacy of local anaesthesia has been well documented in the literature. Amid et al15 reported having utilized local anaesthesia for over 10,000 groin hernia repairs over two decades and found it very safe and useful. There was no anaesthetic related fatality. Obesity posed no problems while using local anaesthesia. We did not encounter any problems while using local anaesthesia. REFERENCES
Copyright 2003 - Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03028t1.jpg] [is03028t2.jpg] |
| |||||||||

{kind=link}
{kind=link}