 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 65, No. 2, March-April, 2003, pp. 182-184 Case Report Benign idiopathic stricture of the duodenum Shivananda Prabhu, Erel A. I. Diaz, Shubha Rao, T. K. Susheel Kumar Department of Surgery, Unit III, KMC Attavar, Mangalore 575 001.
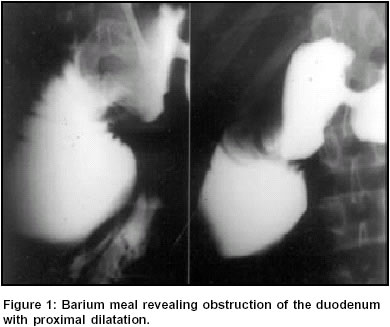
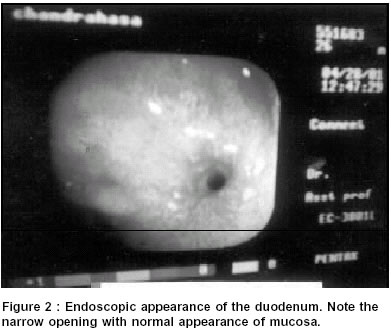
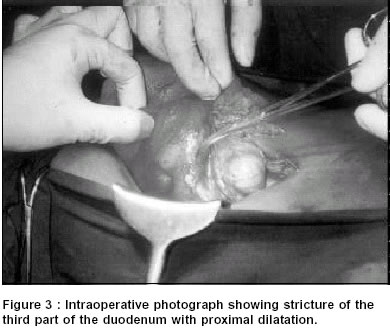
Paper Received: October 2001, Paper Accepted: January 2002. Source of Support: Nil Code Number: is03032 ABSTRACT Benign strictures of the distal duodenum are rare. While idiopathic benign strictures of the ileum and jejunum have been described in the literature, those of the distal duodenum have not been described. We describe a case of benign stricture of the proximal portion of the third part of the duodenum presenting with high intestinal obstruction. An approach to the diagnosis of the underlying conditions causing distal duodenal strictures is outlined. KEYWORDS: Stricture, duodenum, idiopathic How to cite this article: Prabhu S, Diaz EAI, Rao S, Susheel Kumar TK. Benign idiopathic stricture of the duodenum. Indian J Surg 2003;65:182-4. INTRODUCTION Although idiopathic strictures are common in the jejunum and ileum, they are rare in the distal duodenum. We describe a patient with this uncommon entity and outline an approach for a diagnostic work-up for such a problem. CASE REPORT A 25-year-old male patient presented with complaints of abdominal pain, bilious vomiting and loss of weight of 3 months duration. Pain was mainly felt in the epigastrium, was brought on by intake of food and relieved by vomiting. The patient vomited about 4 to 5 times a day and the vomitus contained food mixed with bile. There was no history of haematemesis. The patient had lost about 13 kg over a period of three months. There was no history of altered bowel habits, maelena or pruritus. The patient had received a blood transfusion for anaemia, about one year before this admission. There was no history of tuberculosis. The patient weighed 35 kg and appeared pale. Abdominal examination revealed no abnormality. The patient was investigated for high subacute intestinal obstruction. Routine haematological and biochemical tests and x-rays of the chest and abdomen were normal. Ultrasound of the abdomen revealed mild hepatomegaly. A barium meal (Figure 1) showed a dilated second part of the duodenum with an abrupt cut-off at the proximal portion of the third part. Upper gastrointestinal endoscopy showed an ulcer in the pyloric channel with a dilated second part of the duodenum (Fig 2). On advancing the scope further, a smooth narrowing of the proximal portion of the third part of the duodenum with a pinhole opening was seen. Biopsy taken on repeat endoscopy showed mucosal inflammation with no evidence of tuberculosis or malignancy. A pre-operative diagnosis of duodenal obstruction was made and the patient was taken up for exploratory laparotomy. During laparotomy, a stricture of the third part of the duodenum with proximal dilatation was seen (Figure 3). A thorough exploration of the rest of the abdomen revealed no other abnormality. A side-to-side pyloroduodeno-jejunostomy with truncal vagotomy was done. Post-operatively, the patient was investigated for gastroduodenal tuberculosis by examination of gastric aspirate for acid-fast bacilli (AFB), and was negative. Fasting serum gastrin was normal. Three months following surgery, the patient had put on 15 kg and remained asymptomatic. DISCUSSION Peptic strictures of the duodenum are usually confined to the first 2 cm of the proximal duodenum and have features of gastric outlet obstruction. Strictures in other areas of the duodenum are usually associated with conditions such as the Zollinger-Ellison syndrome, gastro-duodenal tuberculosis, malignancy, Crohn's disease, post-radiation fibrosis, localized ischaemic injury or chronic pancreatitis. Superior mesenteric artery syndrome and congenital anomalies that can present in adulthood, like duodenal membranes, annular pancreas and duodenal duplications, can also cause duodenal obstruction.1 Mycobacterial infection of the duodenum occurs secondary to gastric tuberculosis which is a rare condition.2 This was ruled out in our case by negative tests of gastric aspirate for AFB smear and culture, endoscopic punch biopsy of the lesion and histopathological examination, serum IgG, IgM and IgA for evidence of tuberculosis and a normal chest x-ray. Moreover, post-operatively, the patient had significant gain in his weight. Crohn's involvement of the duodenum is usually associated with the ileal disease.3 This patient had no features suggestive of Crohn's disease. Small intestinal ulcers of unknown origin are termed `non-specific' or `idiopathic'. An annular ulcer if deep and persistent can frequently develop into a fibrous stricture. Most of these lesions present as intestinal obstruction and a significant proportion have anaemia.4,5 In a study reported from the Mayo clinic, it was found that the ileum was the most common site for these lesions followed by the jejunum.6 That series did not report any patients with duodenal strictures. In conclusion, a rare case of idiopathic duodenal stricture is presented. REFERENCES
Copyright 2003 - Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03032f3.jpg] [is03032f2.jpg] [is03032f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}