 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 65, No. 2, March-April, 2003, pp. 184-186 Case Report Hernia uterine inguinale Tejaswini Vallabha, Vaibhav Mudhale, D. H. Biradar Department of Surgery, B.L.D.E.A.S Shri B. M. Patil Medical College, Bijapur, Karnataka 586103
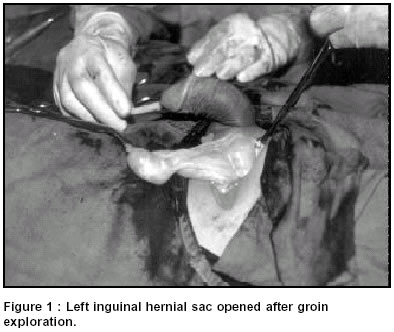
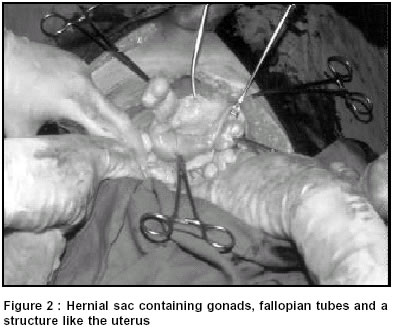
Paper Received: July 2001, Paper Accepted: October 2001. Source of Support: Nil Code Number: is03033 ABSTRACT Herniation of the Mullerian duct derivatives in males is termed hernia uterine inguinale or patent Mullerian duct syndrome. It is a rare syndrome with male pseudohermaphroditism presenting in either neonatal or adult life with inguinal hernia or cryptorchidism or both. Such a case with an unusual cause for haemoperitoneum is presented here with review of literature. KEYWORDS: Hernia uterine inguinale; Patent Mullerian duct syndrome How to cite this article: Vallabha T, Mudhale V, Biradar DH. Hernia uterine inguinale: case report with review of literature. Indian J Surg 2003;65:184-6. INTRODUCTION Hernia uterine inguinale or patent Mullerian duct syndrome is one of the rare causes of male pseudohermaphroditism. These individuals are phenotypically males. They commonly present for inguinal hernia or undescended testis or both. The surgeon unaware of such a condition may go for removal of uterine remnant, damaging blood supply of the abdominal testes. Our patient presented with obstructed hernia and a very unusual cause for haemoperitoneum. CASE REPORT A 25-year-old male patient presented with a painful swelling in the inguinal region and abdominal pain for one day. He had previously noted an inguinal swelling. There was a history of consanguineous marriage of parents. On examination, the patient appeared to be a normally built adult male and was noted to have tachycardia, and guarding and rigidity over the abdomen. He had a left obstructed inguinal hernia. Both the testes were absent from the scrotal sac which was well developed. The penis was normal. The right inguinal canal was empty. A provisional diagnosis of left strangulated inguinal hernia and cryptorchidism was made. The routine investigations were normal, except for presence of free fluid in the abdomen. The left inguinal canal was explored via a groin incision and the hernial sac was opened after isolating it. As the obstruction was released, there was a gush of blood from within the hernial sac. (Figure 1). The sac was found to contain gonads, fallopian tubes and a structure like the uterus (Figure 2). All these were reduced. Omentum was adherent in the sac with the neck being plugged with it. A laparotomy was undertaken which showed about 1.5 litres of blood with active bleeding from a tear in the gastro-epiploic arcade because of traction on the omentum. Bleeding was controlled. The rest of the abdomen was normal. Biopsy of the gonads showed features of testicular atrophy. DISCUSSION Herniation of the Wollfian or Mullerian duct derivatives is termed hernia uterine inguinale.1,2 It is a rare syndrome resulting from a defect in the testicular activity. This syndrome can manifest in the form of agonadia or testicular regression, Leydig cell hypoplasia, 17-hydroxylase deficiency or defective anti-Mullerian hormone (AMH) activity and insensitivity of AMH receptors.1,2 These individuals are phenotypically male with 46XY karyotype. These individuals present in the neonatal period, childhood or adulthood with cryptorchidism, or with an inguinal hernia and undescended testis. They have a normal masculine character but are usually sterile. The testicular biopsy may show atrophic changes or may be normal but response to hormonal stimulation with human chorionic gonadotropin (HCG) is poor. Our patient showed signs of testicular atrophy. Yet there are possibilities of the individual being fertile or developing some fertility in adulthood. There may or may not be a history of consanguineous marriage. The uniqueness of these individuals is that they have both Mullerian and Wollfian duct derivatives. Testis, vas and epididymis are closely adherent running along the uterus, fallopian tubes and part of the vagina. This gives rise to difficulty in separating the gonads and the vas from the fallopian tubes and the uterus without damage to the testis and the vas. These testes have propensity to malignancy because they lie within the abdomen. Uterine or vaginal malignancies in these individuals have not been recorded. The investigations usually done are CT scan, ultrasound abdomen for cryptorchidism and serum AMH levels. AMH levels may be normal or low.4 Low or absent levels can be explained by the mutation of the gene coding AMH. Surgical management is mainly aimed at correcting cryptorchidism, which is difficult and may need staged orchidopexy (bilaterally) without damaging the testis, vas and epididymis. It is sometimes advisable not to separate the vas, which is closely adherent to the Mullerian duct derivatives. Excision of tubes, uterus and vagina can be done but are preferably left alone in some cases.3,5 Prognosis depends upon the integrity of the testicular tissue after successful orchidopexy. REFERENCES
Copyright 2003 - Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03033f2.jpg] [is03033f1.jpg] |
| |||||||||

{kind=link}
{kind=link}