 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 65, No. 2, March-April, 2003, pp. 187-189 Case Report An unusual case of intestinal duplication Ramesh M. Punjani Department of Surgery, K J Somaiya Medical College and Hospital, Ayurvihar, Eastern Express Highway, Mumbai 400 077.
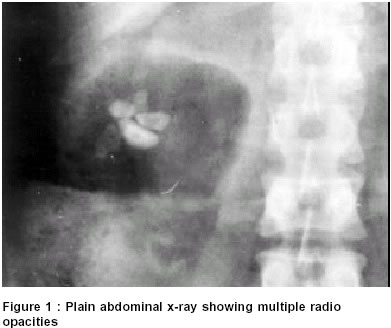
Paper Submitted: September 2001, Paper Accepted: November 2001. Source of Support: Nil Code Number: is03035 ABSTRACT Duplications of the alimentary tract are a rare group of malformations often encountered in childhood. These have varying modes of presentation and can be associated with different diseases. We present a case of intestinal duplication in an adult associated with mesenteric nodal tuberculosis. KEYWORDS: Bowel: duplication, Bowel: tuberculosis How to cite this article: Punjani RM. An unusual case of intestinal duplication. Indian J Surg 2003;65:187-9. INTRODUCTION We present a case of intestinal duplication associated with tuberculosis of the adjoining mesenteric nodes, an unusual association. CASE REPORT A 35-year-old female presented with multiple episodes of colicky periumbilical pain of three years duration. There were no other complaints attributable to the upper or lower gastrointestinal tract. Physical examination was unremarkable as were the routine haematological and biochemical tests. A plain x-ray of the abdomen obtained during an attack of pain had failed to show features suggestive of bowel obstruction but revealed multiple radio-opaque densities surrounded by a gas shadow in the right lumbar region (Figure 1). A barium meal follow-through examination done subsequently was normal. Ultrasonography of the abdomen showed an intra-abdominal cyst containing some calculi on the right side of the abdomen, however, the precise anatomical location of the cyst could not be determined. Before any further investigations could be carried out, the patient presented with an `acute abdomen' and underwent an emergency laparotomy. Abdominal exploration revealed a 10 cm x 8 cm cyst in the distal ileal mesentery about 30 cm proximal to the ileocecal junction. This was found to be a cystic duplication of the ileum attached to the `parent ileum' via a tubular attachment. Multiple enlarged lymph nodes were present in the mesentery. The rest of the small and the large bowel was normal. The cyst, along with the adjacent bowel was resected (Figure 2) and intestinal continuity was re-established with a two- layered end-to-end anastomosis. The cyst appeared to be thick-walled with sloughed out mucosa and contained multiple calcified faecoliths consistent with those observed on the plain x-ray of the abdomen. Histopathology confirmed the cyst to be due to ileal duplication. The adjacent resected ileum was healthy but the mesenteric lymph nodes showed caseating tuberculous granulomas. The patient received a full course of four-drug anti-tuberculous therapy and has done well since. DISCUSSION Duplications of the alimentary tract are a group of rare malformations occurring in 1 out of every 4500 autopsies.1 Although Calder et al published their first report in 1733, Ladd popularised the term `duplication' in 1937.2 Duplications are known to occur along the entire gastrointestinal tract, the commonest site being the small intestine. Many authors have noted the association of intestinal duplications with congenital anomalies in skeletal, gastrointestinal and genitourinary systems.3 Almost 85 per cent of the duplications are diagnosed by the age of two years1 and only rarely do they manifest in adulthood, as in our patient. Common presentations of small intestinal duplications include obscure abdominal pain, volvulus, intussusception and gastrointestinal bleeding. Ultrasonography, CT scan, technetium scan and contrast studies help in the diagnosis of cysts due to the duplication of the small bowel. Often, however, these entities come to light only at exploration.3 Rare instances of malignant changes within these cysts have been reported.4 In our case, the bowel draining into the mesenteric nodes which showed tuberculosis was healthy. As the entire mucosa of the cyst had sloughed out, the cyst wall did not show any granulomas. It is a matter of conjecture whether the duplication cyst harboured tubercle bacilli and was the cause for these lesions. This case highlights an unusual pathological association between a `duplication cyst of the small bowel' and tuberculosis. REFERENCES
Copyright 2003 - Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03035f1.jpg] [is03035f2.jpg] |
| |||||||||

{kind=link}
{kind=link}