 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 65, No. 2, March-April, 2003, pp. 189-190 Case Report Primary extravesical inguinal stone formation after mesh hernioplasty Rajesh Goel, Pawanindra Lal, Rajeev Sharma Department of Surgery, Government Medical College, Chandigarh.
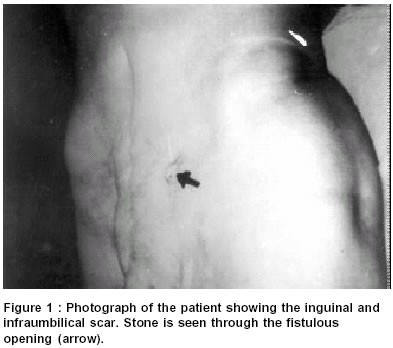
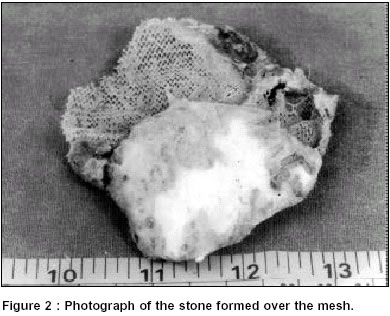
Paper Received: July 2001, Paper Accepted: January 2002. Source of Support: Nil Code Number: is03036 ABSTRACT Foreign body acts as a nidus for stone formation in the urinary tract and such stones form at different sites in the urogenital tract. We report a case, probably the first in literature, of a stone formed outside the urinary bladder over a mesh used for inguinal hernioplasty. The possible mechanism is discussed. This case adds to the list of known complications of one of the commonest operations performed by surgeons. KEYWORDS: Bladder stone, inguinal hernia, foreign body How to cite this article: Goel R, Lal P, Sharma R, Primary extravesical inguinal stone formation after mesh hernioplas. Indian J Surg 2003;65:189-90. INTRODUCTION Inguinal hernia remains one of the commonest operations performed by general surgeons. An accidental deep bite of the bladder resulting in a urinary fistula is documented. However, formation of a stone over the polypropylene mesh outside the bladder in the event of such an injury is as yet unreported in surgical literature. We report this unusual complication. CASE REPORT A 55-year-old male who had undergone a cystolithotomy two years prior, followed by a mesh hernioplasty a year later presented with the leakage of urine from the inguinal scar for 10 days. He reported frequency of micturition and a thinning of his stream for 6 months. Examination revealed midline infraumbilical and inguinal scars. The medial end of the inguinal scar had a retracted fistulous opening of around 1cm x 1cm through which a stone could be seen (Figure 1). The prostate was not enlarged on digital rectal examination and on ultrasonography. A retrograde urethrogram showed a 0.5 cm stricture just distal to the prostatic urethra. The renal functions were deranged with blood urea of 140 mg / dl and serum creatinine of 3.2 mg / dl. Microscopic examination of the urine showed 20-30 pus cells per high power field. Ultrasonography showed bilateral mild hydroureteronephrosis with a thickened bladder wall. Surgical exploration revealed a large stone (7cm x 5cm) formed over the polypropylene mesh (Figure 2) outside the bladder along with a 0.5cm diameter opening in the anterior wall of the bladder through which urine was leaking. The stone along with the mesh were removed. The bladder was explored by extending the fistulous opening and was closed in layers and a suprapubic catheter (SPC) was introduced at a separate site. Postoperatively the patient received intravenous antibiotic therapy for organisms isolated by culture of urine and their sensitivity. The patient recovered uneventfully and the renal function returned to normal. The urethral stricture was managed with repeated dilatations over the next 12 weeks. The suprapubic catheter was removed after 4 months and the patient had a normal voiding on the last follow-up. DISCUSSION Stone formation over a foreign body inside the bladder is well documented.1 This had been reported earlier after laparoscopic herniorrhaphy.2 Primary vaginal calculus after pelvic surgery has also been reported.3 Primary extravesical stone formed over a foreign body like a polypropylene mesh as seen in our patient has not been reported earlier. The mechanism of stone formation in our case was possibly `a bite' of the bladder wall during fixation of the mesh at the medial end in the hernioplasty. This would have led to the formation of a sinus in the bladder wall resulting in leakage and collection of urine in the extravesical space over a period of several months. Subsequent stone formation may have then occurred in the stagnant urine outside the bladder because the hole in the bladder wall was found to be quite small. Pressure atrophy due to the enlarging stone of the subcutaneous tissue may have led to the vesicocutaneous fistula. This case is reported for its unique presentation and as an addition to the list of complications after inguinal hernioplasty. REFERENCES
Copyright 2003 - Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03036f1.jpg] [is03036f2.jpg] |
| |||||||||

{kind=link}
{kind=link}