 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 65, No. 2, March-April, 2003, pp. 191-192 Case report Chronic progressive penile strangulation with urethrocutaneous fistula-report of a case Iqbal Singh, G. Nabi, M. S. Ansari, Gulshant Panesar Department of Urology, All India Institute of Medical Sciences, New Delhi-110 029.
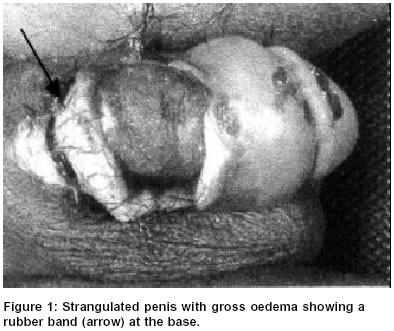
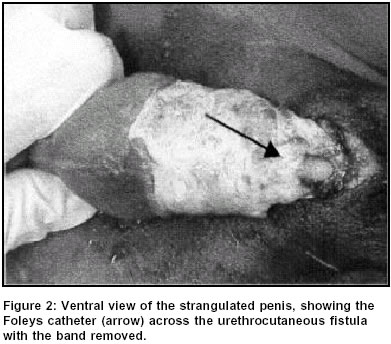
Paper Received: June 2001, Paper Accepted: May 2002. Source of Support: Nil Code Number: is03037 ABSTRACT We report a case of a self-inflicted chronic progressive penile strangulation leading to the formation of urethrocutaneous fistula in a mentally deranged 12-year-old boy. The literature regarding the occurrence, mechanism and management of this entity is discussed. KEYWORDS: Penis, ischaemia, gangrene, fistula, urethrocutaneous How to cite this article: Singh I, Nabi G, Ansari MS, Panesar G. Chronic progressive penile strangulation with urethrocutaneous fistula. Indian J Surg 2003;65:191-2. INTRODUCTION Penile incarceration, tourniquet and strangulation injuries are known to occur in adults as well as children. We report a case of self-inflicted chronic progressive penile strangulation leading to ischaemia and urethrocutaneous fistula caused by a rubber band in a mentally deranged 12-year-old boy. The literature regarding the occurrence, mechanism and management of this entity is discussed. CASE REPORT A 12-year-old circumcised boy presented to the outpatient department with penile oedema, ulceration, suppuration and gangrene with perineal urinary leak. On examination the entire organ was swollen and ischaemic with markedly diminished distal sensations and superficial distal penile gangrene. There was ulceration of the ventral shaft of the penis at the base where a constricting rubber band was found buried. A urethral fistula was present at the site (Figure 1). History revealed that the boy was suffering from cerebral leukodystrophy. The injury was caused by the application of an elastic band by the patient three days prior to his seeking help. The patient was successfully managed by releasing the constricting rubber band, debridement of the wound and a careful per-urethral catheterization. A Foleys catheter was used to splint the urethrocutaneous fistula and allow healing of the transected corpus spongiosum and urethra (Figure 2). A formal suprapubic cystostomy and urethral repair was deferred due to poor local hygiene and ischaemia. The catheter was removed after 2 months and he voided normally and at a further follow-up of 3 months, the fistula had closed completely but the patient developed a mild passable stricture with localized spongiofibrosis. This was successfully managed by a regular two-monthly endoscopic dilatation. The patient's attendants were taught to perform a monthly urethral calibration and dilatation on a domiciliary basis to maintain urethral patency. He was subsequently lost to follow-up. DISCUSSION Neglected penile tourniquet injuries may be devastating and may culminate in frank ischaemia with penile gangrene and amputation. Though literature abounds with several reports of penile strangulation caused by rings, nuts, hair, threads and bands, their removal and management is often not straightforward.1,2 Though hair appears to be one of the commonest strangulating agents2,3 a rubber band was the strangulating agent in our case. The present case had a slow progressive ischaemia of the penis due to the dynamic elastic tension in the applied rubber band. This resulted in chronic penile engorgement, lympho-venous oedema, ischaemia and sloughing of the corpus spongiosum and urethra leading to a fistula. Pressure necrosis of the thin ventral skin and urethra resulted in slackening of the tension in the rubber band. The corpora cavernosa escaped severe injury due to the dense fibrous tunica albuginea which envelops it. Acute urinary retention did not occur as the patient continued to void both from the external meatus as well as from the urethral fistula. Though grade four injuries must be managed by suprapubic urinary diversion and delayed urethral reconstruction, our case did well with an initial simple urethral catheterization. In the pregangrenous stage, penile degloving, corporal aspiration and heparinization may be needed to restore pulsations distal to the strangulation. Penile Doppler flowmetry and penile arteriography and/or fluroscein angiography may aid in the evaluation of the ischaemic penis following the release of the strangulated penis. In frank autoamputation penile microsurgical reimplantation may salvage the victim if brought in time.5 Progressive chronic dynamic ischaemic compression injuries such as those caused by elastic rings, may result in partial tissue devitalization with simultaneous tissue healing and hence the outcome may not always be disastrous. An immediate urinary diversion or outlet should be provided in all such cases at the earliest. Due to the precarious blood supply, a staged formal urethral repair can be undertaken later. Urethral stricture and impotence are some of the delayed complications of this condition.4 Such self-inflicted injuries in children may denote an underlying psychological abnormality or they may have been used to prevent enuresis and incontinence by the mentally deranged child or may be a result of child abuse.2 Awareness of this pathology in any case of penile oedema and gangrene can prompt an early diagnosis. Prompt attention to asepsis and immediate catheterization and/or urinary diversion may reduce morbidity in such unfortunate children. REFERENCES
Copyright 2003 - Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03037f1.jpg] [is03037f2.jpg] |
| |||||||||

{kind=link}
{kind=link}