 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
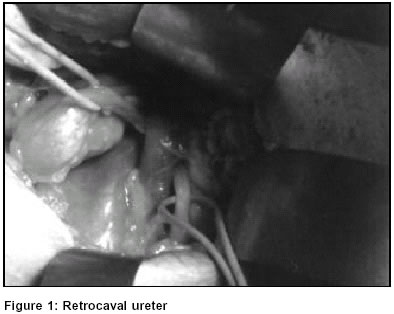
Indian Journal of Surgery, Vol. 65, No. 2, March-April, 2003, pp. 198 Images in Surgery Retrocaval ureter Anand Prakash, A. K. Mishra, O. P. Agrawal Department of Surgery, Bokaro General Hospital, Bokaro Steel City
Paper Received: August 2002, Paper Accepted: November 2002. Source of Support: Nil Code Number: is03040 How to cite this article: Prakash A, Mishra AK, Agrawal OP. Retrocaval ureter. Indian J Surg 2003;65:198. Case Report A 44-year-old man presented with dull intermittent right lumbar pain. Routine examination of urine and plain abdominal x-ray were normal. Ultrasonography and intravenous urogram (IVU) showed hydronephrosis and upper hydroureter with a "J" deformity on the right side. Retrograde pyelography (RGP) of the right side showed a tortuous, dilated ureter in the shape of an italic S, beginning just above the pelvic brim and ending below the renal pelvis. Ureteric catheter could not be passed up to the renal pelvis. Operation done by a right lumbar approach showed a retrocaval ureter. The dilated caudal ureteric segment was excised. The ureter was then reanastomosed to the proximal dilated segment anterior to the inferior vena cava. COMMENT Retrocaval ureter is a rare congenital anomaly in which the right ureter passes behind the inferior vena cava with varying degree of ureteral compression. This occurs due to the persistence of the posterior cardinal vein. Two varieties of retrocaval ureter have been described. The low loop (type I) is commoner as compared to the high loop variety (type II). The anomaly develops almost exclusively on the right side except in patients with situs invertus. The anomaly occurs more commonly in males and the onset of symptoms is usually in the fourth decade of life. Presentation is commonly with dull right lumbar pain or urinary tract infection. The typical ureteric deformity on IVU and RGP. A CT scan may of value in establishing the diagnosis. Patients without symptoms or hydronephrosis should be observed. Those with hydronephrosis and upper hydroureter, a dismembered pyeloplasty with anterior transposition of ureter and re-anastomosis is the treatment of choice. Nephrectomy may be required in presence of marked hydronephrosis and cortical atrophy if the contralateral kidney is normal. Copyright 2003 - Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03040f1.jpg] |
| |||||||||

{kind=link}