 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 65, No. 3, May-June, 2003, pp. 241-245 Duodenogastric reflux before and after cholecystectomy: evaluation by Technetium-99m Mebrofenin scintigraphy Nadeem Ahmad Bhat, Khurshid Aalam Wani, Shoukat Hussain Khan,* Nazir Ahmad Wani, Mushtaq Ahmad Syed* Departments of General Surgery and *Nuclear Medicine, Sher-i-Kashmir Institute of Medical Sciences, Srinagar.
Paper Received: September 2002 Paper Accepted: January 2003. Source of Support: Nil Code Number: is03046 ABSTRACT The present study was conducted prospectively in the department of General Surgery and Nuclear Medicine, SKIMS from April 1999 to March 2000. 30 patients with symptoms attributable to ultrasound-documented gallstones were included in the study. 5 mci Tc-99m Mebrofenin was used for scanning the hepatobiliary system on a Siemens Icon-Gamma Camera with predefined computer software. The stomach was localized using Tc-99m sulphur colloid. In the present study 16 patients did not reveal any significant reflux pre and postoperatively. Seven (23.3 per cent) patients who had a significant duodenogastric reflux preoperatively persisted with significant postoperative reflux as well, however, the quantitative difference in reflux was insignificant (p > 0.05). Seven (23.3 per cent) patients who had an insignificant preoperative reflux developed a significant postoperative reflux (p < 0.05). These patients also had post-cholecystectomy symptoms attributable to alkaline gastritis. Tc-99m Mebrofenin hepatobiliary scanning with gastric localization is a useful, non-invasive, reproducible and cost-effective method to evaluate duodenogastric reflux both pre and postoperatively. Most of the drawbacks encountered with other methods, especially those needing gastric intubation, are overcome. How to cite this article: Bhat NA, Wani KA, Khan SH, Wani NA, Syed MA. Duodenogastric reflux before and after cholecystectomy: Evaluation by Technetium-99m Mebrofenin scintigraphy. Indian J Surg 2003;65:241-5. INTRODUCTION Enterogastric reflux is an important factor in the pathogenesis and symptomatology of several upper gastrointestinal tract disorders including gastritis, oesophagitis and gall stone dyspepsia.1 Not all patients undergoing cholecystectomy are
cured of their symptoms by cholecystectomy. About
20-40 per cent of such patients continue to have a variety
of gastrointestinal symptoms.2 In a significant number
of patients there is no obvious cause for post-cholecystectomy complaints, and they are believed
to have symptoms attributable to cholecystectomy. However, there is much experimental and
clinical evidence that gall bladder disease and
cholecystectomy can increase duodenogastric reflux (DGR). DGR to
some extent is a physiological event which may assume
a pathological role after cholecystectomy due to loss
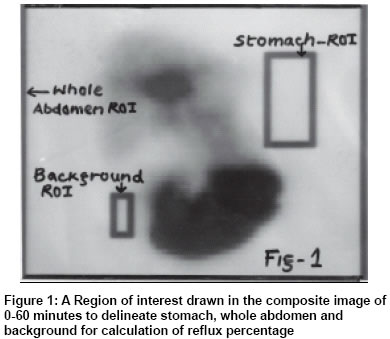
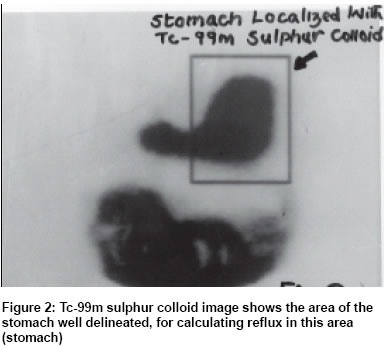
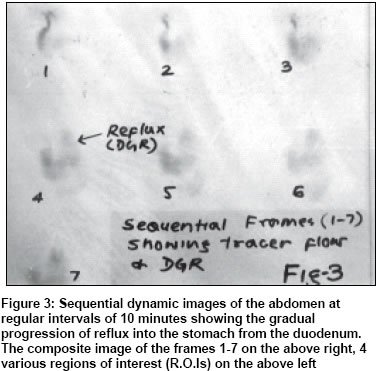
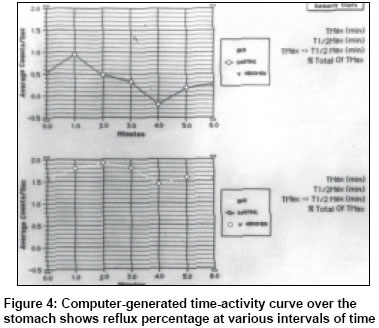
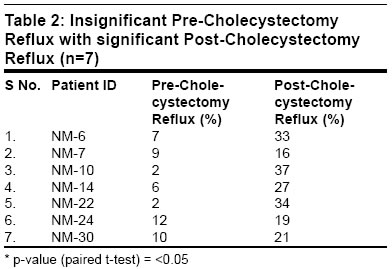
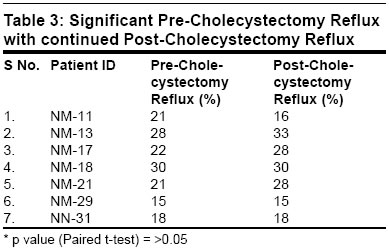
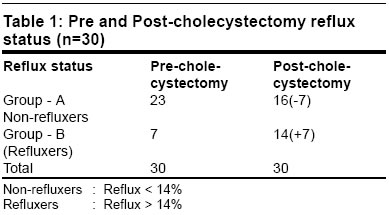
of Objective physiological measurement of DGR is difficult and until recently most of the methods used for measuring DGR have required intubation, which in addition to being an invasive technique may itself promote DGR and lead to spurious results. In cholescintigraphy the contents of the duodenum are rendered visible with a hepatobiliary tracer that is excreted through the liver and transported to the duodenum. The movement of the tracer can be recorded with a Gamma Camera interfaced with a computer. In sequential pictures the tracer can be followed from the biliary tree into the duodenum and jejunum and in case of DGR into the stomach. Background-subtracted time activity curves over regions of interest (ROI) covering the whole abdomen and stomach, make quantitative estimation of the DGR possible (Figure 1). MATERIAL AND METHODS Thirty patients (4 males, 26 females) with a mean age of 40 years (range 17-55 years) have been included in the study. Abdominal pain, postprandial fullness, fatty dyspepsia, nausea and vomiting were the predominant presenting symptoms. 29 patients underwent a standard cholecystectomy through a right subcostal incision and one patient underwent laparoscopic cholecystectomy. The postoperative period was uneventful in 27 patients. Three patients developed postoperative wound infection which was effectively managed by antibiotics and antiseptic dressings. None of these patients had any other prior gastric or hepatobiliary surgery. All these patients underwent a pre and postoperative cholescintigraphy to document and quantify DGR. Postoperative cholescintigraphy was done between 2 to 4 months after cholecystectomy. Prior to the scan, all drugs liable to affect the upper gut motility were stopped for 48 hours. The patients refrained from smoking and fasted for 4-6 hours before the scan. All the patients were injected with 5 mci (millicuries) of Technetium-99m Mebrofenin (an iminodiacetic acid derivative) intravenously. The patient waited for 30 minutes to allow hepatic uptake and clearance. To stimulate a DGR the patient was instructed to drink 250 ml of milk which was at room temperature. Cholescintigraphy was carried out on a Gamma Camera (SIEMENS-ORBITER) with a large field of view and fitted with a LEAP (Low-Energy All Purpose) parallel hole, collimator and interfaced to a computer (SIEMENS-ICON). Standing images of the whole abdomen were acquired using a predefined dynamic programme. 7 serial images of 60 seconds duration each were acquired on a matrix size of 64 x 64, at an interval of 10 minutes with patient sitting during the interval period. At the completion of the dynamic images the patient drank 5 mci of Technetium-99m labelled sulphur colloid in sterile water to map the gastric area. A 2-minute image on a matrix size of 128 x 128 was acquired (Figure 2). The dynamic images (Figure 3) were processed on the computer. A composite image of all the 7 frames (0-60 minutes) was constructed (Figure 1). Regions of interest (ROI) were drawn for the whole abdomen, stomach and the background. The stomach ROI was drawn using the static Tc-99m sulphur colloid image as reference. Every effort was made to avoid overlap of other regions, especially the liver. The background ROI was selected from the region adjacent to the gut. From the computer-generated time activity curve the background corrected percentage activity (reflux) in the stomach area was calculated (Figure 4). Reflux activity in the range of 1-14 per cent was considered insignificant and attributed to background activity,5 or to activity in the liver that might be overlapped by gastric ROI or to overlap of small bowel into gastric ROI6 or to normally occurring physiological reflux.7 A partial `t' test was applied to find the significance of difference in reflux (%) before and after cholecystectomy. Testing by this method eliminates individual sampling variations because the sample is one and the observations on each patient in the sample are taken before and after the cholecystectomy (Table 2 and Table 3). p < 0.05 was considered significant at 95 per cent confidence interval. RESULTS The DGR was calculated as a percentage of total abdominal activity. An insignificant (< 14 per cent) pre-cholecystectomy DGR was identified in 23 (76.66 per cent) patients. 7 patients had a significant (>14 per cent) pre-cholecystectomy reflux. These patients (Group B, Table 1) were labelled as pre-cholecystectomy refluxers, and they continued to have a post-cholecystectomy reflux with 4 patients showing an increased reflux, which was statistically insignificant (p>0.05, Table 3). 7 of the 23 patients (Group A, Table 1) who showed insignificant pre-cholecystectomy DGR developed postcholecystectomy reflux ranging from 16-37 per cent (Figure 4) and the degree of reflux was found to be statistically significant (p<0.05). Overall, in the study group of 30 patients, 14 patients had a significant post-cholecystectomy reflux, however, 7 (50 per cent) of them had a pre-cholecystectomy reflux as well. It was only in the remaining 7 patients that a significant reflux developed after cholecystectomy. DISCUSSION The scintigraphic method to demonstrate DGR using Tc-99m Mebrofenin is physiological and cost-effective. In tracer amounts the biliary radiopharmaceutical agent causes no alteration in the bile salt metabolism and dynamics. In cholescintigraphy, the contents of the duodenum are rendered visible with a hepatobiliary tracer that has an identical physiological behaviour to bilirubin and is excreted through the liver into the duodenum. The hepatobiliary tracer kinetics using Tc-99m Mebrofenin can be recorded by a Gamma camera interfaced to a computer. For ease of identification, a stomach localization scan using Tc-99m sulphur colloid is used (Figure 2). In sequential frames the radiotracer can be followed from the biliary tree into the duodenum and jejunum and in case of DGR into the stomach. The reflux can be quantified using predefined software which involves marking the regions of interest and generating background subtracted time activity curves. Unlike other invasive techniques there is no chance of inducing a reflux by the procedure itself. Patients who have symptoms because of DGR prior to cholecystectomy are unlikely to benefit from cholecystectomy. 7 patients (23.3 per cent) who had significant preoperative DGR continued to have the symptoms and the symptoms even worsened due to increased DGR in 4 patients from this group of preoperative refluxers. The post-cholecystectomy symptoms of patients who had significant DGR did not differ much from patients who did not have a significant DGR. However, one major difference which we noted in our study was that bilious vomiting was present in 6 patients postoperatively. These included 4 patients who had bilious vomiting preoperatively and 2 patients who developed it postoperatively. 3 patients who had gastritis preoperatively continued with it postoperatively and 2 developed gastritis denovo. DGR has been implicated in the causation of gastritis in other studies also.8 The incidence of DGR in our study increased from 23.3 per cent to 46.6 per cent postoperatively. CONCLUSION Tc-99m Mebrofenin (HIDA) scanning of the hepatobiliary system is a reasonable and reliable method for the quantitative evaluation of duodenogastric reflux (DGR). Most of the drawbacks encountered with other methods, especially with those needing gastric intubation, are overcome. Gallstones may be associated with dyspepsia without any aetiological relationship and surgery might be of little help to such patients. Preoperative hepatobiliary scanning of gallstone patients may be done for the evaluation of DGR which can be responsible for persistent symptoms after cholecystectomy. Patients with significant DGR may need further evaluation and should be made aware of the possibility of persistent symptoms or of the appearance of new symptoms after cholecystectomy. In patients with post-cholecystectomy symptoms, such scintigraphy can help in identifying DGR as a cause when others have been ruled out. In light of our observations in this study, we would recommend a Tc-99m Mebrofenin cholescintigraphy in all symptomatic patients, pre and post-cholecystectomy as this would help in evolving an optimal management policy and also in understanding the pathophysiology of such patients. REFERENCES
Copyright 2003 - Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03046f1.jpg] [is03046t1.jpg] [is03046f3.jpg] [is03046f4.jpg] [is03046t3.jpg] [is03046t2.jpg] [is03046f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}