 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 65, No. 3, May-June, 2003, pp. 246-250 Thoraco-abdominal flap cover for large post-mastectomy defects S. V. S. Deo, Joydeep Purkayastha, Nootan K. Shukla, Sonal Asthana Department of Surgical Oncology, Institute Rotary Cancer Hospital, All India Institute of Medical Sciences, New Delhi 110029, India.
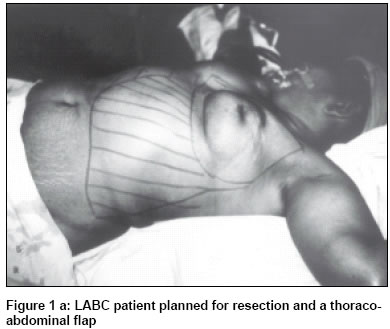
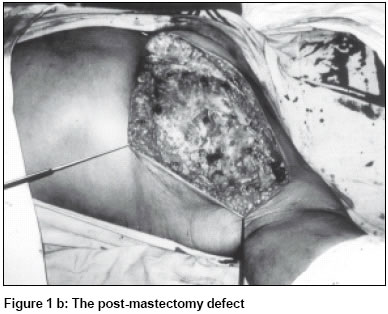
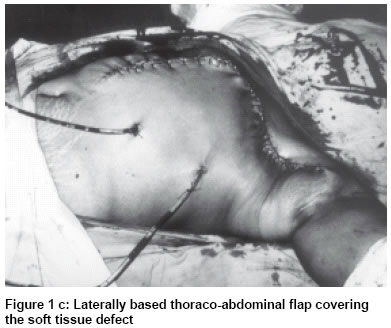
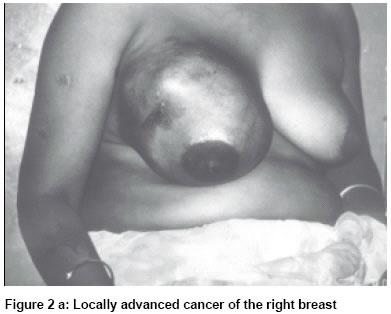
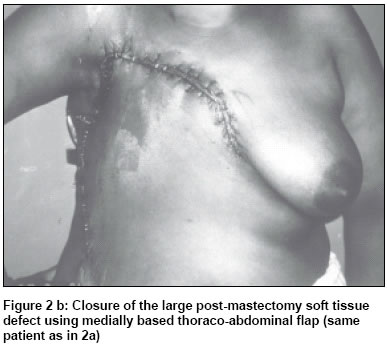
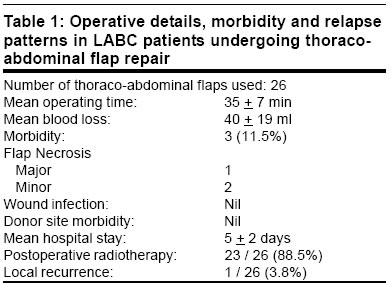
Paper Received: June 2002. Paper Accepted: November 2002. Source of Support: Nil Code Number: is03047 ABSTRACT: The majority of breast cancer patients in India present with advanced disease, in whom radical surgical extirpation produces large defects that may not be suitable for primary closure. The primary aim in such cases is to achieve an adequate soft tissue cover expeditiously. Various methods have been tried in the past, however, there is no consensus regarding the method of choice in such situations. A retrospective analysis of the breast cancer database of a single surgical unit was done to find out an ideal surgical option in an Indian setting. Forty-five (12.8 %) out of 350 locally advanced breast cancer patients undergoing mastectomy required additional surgical procedures for soft tissue cover. Thoraco-abdominal (TA) flap was utilized for cover in 26 (7.4 %) patients. For patients undergoing TA flap repair, the mean operating time was 35 min, blood loss was 40 ml and hospital stay was 5 days. Only 1 out of 26 patients had a major wound problem, 23 patients received postoperative radiation and only 1 patient developed a local recurrence. The current study has shown encouraging results with TA flap and in view of its simplicity we recommend that TA flap should be used as a first option flap in patients with large post-mastectomy defects. KEY WORDS: Locally advanced breast cancer, Post-mastectomy defects, Thoraco-abdominal flap (TA flap). How to cite this article: Deo SVS, Purkayastha J, Shukla NK, Asthana S. Thoraco-abdominal flap cover for large post-mastectomy defects. Indian J Surg 2003;65:246-50. INTRODUCTION Breast cancer is the commonest malignancy in women all over the world and is a leading cause of death from cancer in females.1 In the developing world, it may account for 300,000 cases and 150,000 deaths annually.2 Locally advanced breast cancer (LABC) accounts for 10%-25% of all breast cancer in developed countries whereas 40%-50% of breast cancer patients in developing countries like India present with locally advanced disease.1,2 Surgery plays an important role in the overall management of LABC and radical surgical resection may result in large soft tissue defects necessitating an additional surgical procedure to achieve adequate soft tissue cover. Several methods have been tried in the past including skin grafts, local flaps, omental flaps, abdominal flaps and myocutaneous flaps to cover such soft tissue defects.3-6 The primary aim of reconstruction in this group should be an expeditious and simple closure with good quality skin cover, rapid postoperative recovery and short hospital stay so that the patients can receive early postoperative radiotherapy and chemotherapy.6 There is no clear consensus on the method of repair to be adopted in such cases. The method of choice depends upon the treatment facilities available and the expertise of the surgeon. There is a need to evolve a simple and reliable surgical procedure so that a large number of Indian surgeons dealing with breast cancer can treat LABC more effectively. In an attempt to address the above issues we present our experience of Thoraco-abdominal (TA) flap cover for large post-mastectomy defects. MATERIAL AND METHODS A retrospective analysis of the breast cancer database of a surgical unit based in a tertiary care cancer centre was done. In the period between 1993 and 2002, a total of 850 breast cancer patients were operated upon, of which 350 patients had LABC. A total of 45 (12.8 %) patients of LABC required flap cover for closure of large soft tissue defects following radical resection. Between 1993 and 1997 myocutaneous flaps were used in 18 patients and split skin graft in 3 patients. Since 1998 we have been using TA flap for closure of large post-mastectomy defects. TA flap was used in 26 (7.4 %) patients of LABC between 1998 and 2002. The medical records of patients undergoing TA flap cover were reviewed and analyzed to assess operative duration, blood loss, postoperative morbidity, hospital stay, adjuvant treatment and follow-up details. The Thoraco-abdominal (TA) flap utilizes the skin and subcutaneous tissue of the upper antero-lateral abdominal wall.7 It is a rotation advancement type of fasciocutaneous flap (Type-c). It is based on two sets of direct perforating segmental arteries arising from the subcostal, lumbar and deep epigastric arcades. There are two sets of perforating branches the lateral, arising from the lumbar and subcostal arteries at the level of the anterior border of the latissimus dorsi muscle and the medial, arising from the deep epigastric arcade at the lateral border of the rectus abdominis muscle.7,8 These two vascular systems are connected through a subfascial anastamosis.8,9 For post-mastectomy defects on the lateral side of the chest wall and the axilla, a medially based flap based on the medial perforating branches can be used whereas for medial soft tissue defects of the chest wall, a laterally based flap based on the lateral perforators is preferable. The plane of dissection should be maintained superficial to the rectus fascia and external oblique aponeurosis, which is relatively avascular. The limits of the flap are the midline medially (for lateral based flap), and the mid-axillary line laterally (for medially based flap), and the lower extent varies from patient to patient depending upon the built and skin requirement. The lax abdominal skin can be adequately mobilized to effect primary closure of the donor site. After completion of the mastectomy and assessing the defect, the TA flap is marked, maintaining a strict length-breadth ratio of 1:1 within the vascular territory as described above. The dissected flap can be advanced and rotated into the defect without tension. The tip of the flap is trimmed in patients with doubtful viability and the wound closed using 2-0 nylon interrupted sutures after placing two closed suction drains one draining the mastectomy site and the other draining the donor area. MS Access database program and SPSS statistical software package, version 9 was used for data storage and analysis. RESULTS TA flap was used to cover large post-mastectomy defects in 26 (7.4%) out of 350 patients with LABC following radical surgical resection. There were 25 female and 1 male patient. Radical mastectomy was performed in 8 and modified radical mastectomy was performed in 18 patients. A complete axillary dissection including level I, II and III nodes was performed in all the patients. In 24 out of 26 patients, laterally based TA flap (Figure 1a, 1b, 1c) was used to cover predominantly medial chest wall defects while in 2 patients with lateral defect, medially based TA flap was used (Figure 2a, 2b). The operative duration, blood loss, hospital stay, flap morbidity, postoperative radiotherapy details and recurrence patterns in LABC patients who had TA flap cover are shown in Table 1. Postoperative radiotherapy (50Gy / 25Fr / 5 weeks) was planned for all the patients; however, 2 patients defaulted radiotherapy and 1 could not receive radiotherapy in view of major wound problem. All the patients received 6 cycles of anthracycline based chemotherapy and hormonal therapy (Tamoxifen) was given in ER and PR positive patients. DISCUSSION The majority of breast cancer patients in developing countries like India present with locally advanced disease.1,2 Surgical resection is an integral part of the multimodality management of LABC. Radical resection in such patients often results in large, soft tissue defects of the chest wall, which are not suitable for primary closure. Additional surgical procedures are often required to manage large post-mastectomy defects. Since a majority of these patients also require adjuvant radiotherapy and chemotherapy, the primary objective in case of such patients is to provide a simple, expeditious and reliable skin cover with minimal morbidity and hospital stay. In view of the guarded prognosis and the need for early institution of chemoradiotherapy, complex reconstructive procedures to recreate the breast mound are generally not offered to these patients.10 Various surgical procedures have been used during diferrent time periods. Until skin grafting became available radical mastectomies were allowed to heal by secondary epithelialization.3 Skin grafting was utilized for post-mastectomy cover in the 50s, when radical mastectomy was the treatment of choice.4 The major drawbacks of split skin grafting are poor cosmesis, secondary infection, increased donor and recipient site morbidity and late loss following radiation.4,6 Omental transposition with skin grafting for coverage of post-mastectomy defects has been reported in the literature. Lopez et al11 have reported a success rate of 76% and an abdominal herniation rate of 8% in 50 patients undergoing omental transposition for advanced breast cancer. In a recent series, Cheung et al12 have reported a 100 % success rate and a mean hospital stay of 16 days in breast cancer patients undergoing omental transposition. Basically, omentum provides a healthy bed for skin grafting. The major drawbacks of omental flap are the addition of a laparotomy procedure and the necessity of a split skin graft leading to increased morbidity.13 Myocutaneous (MC) flaps revolutionized the field of reconstructive surgery during the last three decades. Ignio Tansini used the latissimus dorsi (LD) myocutaneous flap first in 1896 for covering a post-radical-mastectomy defect.14 Between 1920 and 1974 this procedure was completely abandoned as Halstead thought this to be unnecessary and hazardous.15 Subsequently, LD flap was reintroduced in 1975 for cover as well as for reconstruction and from 1977 to 1982, LD myocutaneous flap was the most popular method.15,16 Hartramp's Transeverse rectus abdominis myocutaneous flap (TRAM) was introduced in 1982.17 In view of better cosmetic results, reliability and positional advantage, rectus based flaps became more popular than LD flap during the 1980s and 90s.18 The major drawbacks of a myocutaneous flap are requirement of surgical expertise, prolonged operative time and hospitalization, increased blood loss and morbidity. Many Indian surgeons practising breast cancer surgery are not equipped to execute such complex procedures and plastic surgical expertise is not widely available in India. Myocutaneous flaps are currently being used mainly for breast reconstruction in early breast cancer patients in a few specialized cancer centres. The thoraco-abdominal (TA) flap was first described by Brown et al in 1975.7 It has been used for breast reconstruction along with a prosthesis and soft tissue cover following surgery for LABC in some studies during the late 70s and early 80s.6-9 However, with the advent of the myocutaneous flaps in the 80s, TA flap usage declined significantly. TA flap is a Type-c fasciocutaneous flap and the skin and fat of the upper abdomen are used based on medial or lateral perforating vessels.7 Due to the limitations of the myocutaneous flap and skin grafts in LABC patients, we explored the option of TA flap cover in an LABC patient in 1998. In view of the early encouraging results we changed our policy and started using TA flap routinely to cover large post-mastectomy defects. The mean operating time of TA flap was 35 min and blood loss was 40 ml. Whereas a myocutaneous flap, on an average, takes 120 min and the blood loss varies from 200 to 250 ml. Other significant advantages of TA flap are short hospital stay (mean 5 days) and low morbidity. Only 1 patient with uncontrolled diabetes had major flap loss in our series. Since TA flap provides good quality vascularized skin cover, all the patients tolerated postoperative radiation without major wound morbidity. Our experience has also shown that large post-mastectomy defects, extending vertically from the infraclavicular area to the inframammary crease and horizontally from the midline to the mid-axillary line, could be easily covered using a TA flap. Availability of the TA flap option facilitated radical resections with adequate skin margins in LABC patients resulting in a very low local recurrence rate in the current study . To conclude, approximately 12.8 % of LABC patients require some additional surgical procedure to cover large post-mastectomy defects. Many LABC patients in developing countries like India are not being offered the option of radical resection due to lack of a simple and reliable reconstructive surgical option. The other option, of neo-adjuvant chemotherapy, for downstaging followed by surgery is expensive, time-consuming and not widely available. Till date split skin grafts and myocutaneous flaps are the common methods employed. The current study has shown superior results with TA flap and in view of its simplicity and better results we recommend that TA flap should be used as a first option flap in patients with large post-mastectomy defects. We also feel that the majority of general surgeons practising breast cancer surgery in India can easily master the TA flap technique and contribute significantly to the betterment of LABC management. REFERENCES
Copyright 2003 - Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03047f2b.jpg] [is03047f1c.jpg] [is03047f1a.jpg] [is03047f2a.jpg] [is03047f1b.jpg] [is03047t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}