 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 65, No. 3, May-June, 2003, pp. 251-259 Hypothalamic digoxin and inflammatory bowel disease Ravi Kumar Kurup, Parameswara Achutha Kurup Department of Medicine, Medical College Hospital, Trivandrum, Kerala, India and Metabolic Disorders Research Center, Trivandrum,
Kerala, India.
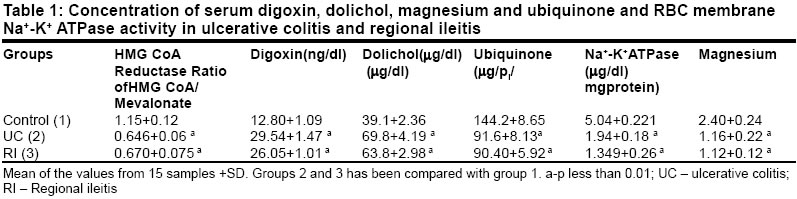
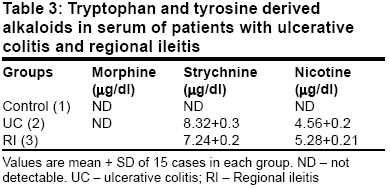
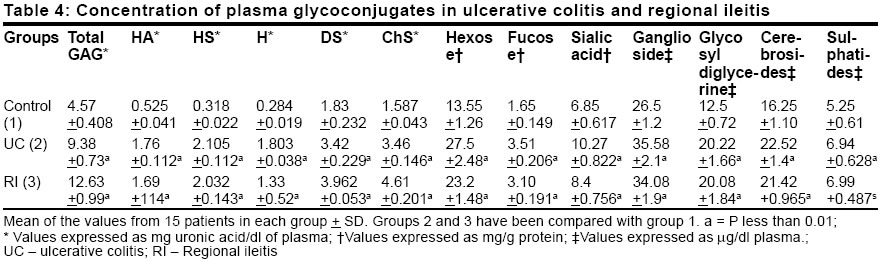
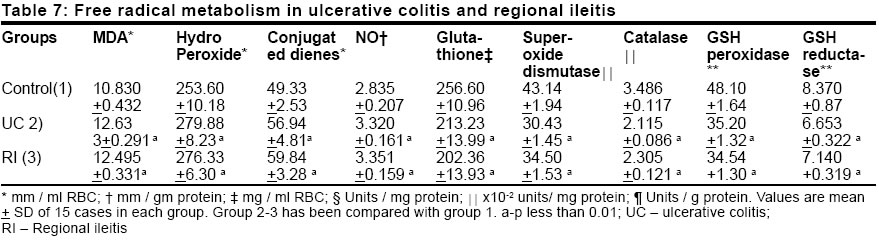
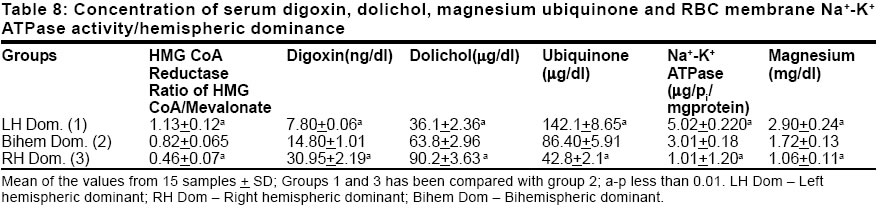
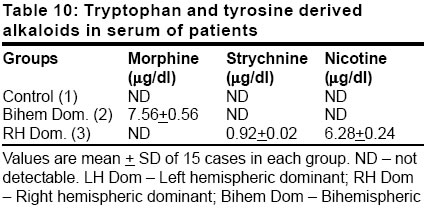
Paper Received: March 2001. Paper Accepted: July 2002. Source of Support: Nil Code Number: is03048 ABSTRACT The isoprenoid pathway produces three key metabolites - endogenous digoxin, dolichol and ubiquinone. It was considered pertinent to assess the pathway in inflammatory bowel disease (ulcerative colitis and regional ileitis). Since endogenous digoxin can regulate neurotransmitter transport, the pathway and the related cascade was also assessed in individuals with differing hemispheric dominance to find out the role of hemispheric dominance in its pathogenesis. The following parameters were measured in patients with inflammatory bowel disease and in individuals with differing hemispheric dominance - 1. plasma HMG CoA reductase, digoxin, dolichol, ubiquinone and magnesium levels, 2. tryptophan/tyrosine catabolic patterns, 3. free radical metabolism, 4. glycoconjugate metabolism, and 5. membrane composition and RBC membrane Na+-K+ ATPase activity. Statistical analysis was done by `ANOVA'. In patients with inflammatory bowel disease there was elevated digoxin synthesis, increased dolichol and glycoconjugate levels, and low ubiquinone and elevated free radical levels. There was also an increase in tryptophan catabolites and a reduction in tyrosine catabolites. There was an increase in the cholesterol: phospholipid ratio and a reduction in the glycoconjugate level of RBC membrane in this group of patients. The same biochemical patterns were obtained in those with right hemispheric dominance. Inflammatory bowel disease is associated with an unregulated isoprenoid pathway and elevated digoxin secretion from the hypothalamus. This can contribute to immune activation, defective glycoprotein bowel antigen presentation and autoimmunity, and a schizophreniform psychosis, important in its pathogenesis. Inflammatory bowel disease occurs in right hemispheric dominant individuals. KEY WORDS: Inflammatory bowel disease, Digoxin, Dolichol, Ubiquinone, Hemispheric dominance. How to cite this article: Kurup RK, Kurup PA. Hypothalamic digoxin and inflammatory bowel disease. Indian J Surg 2003;65:251-9. INTRODUCTION Inflammatory bowel disease (IBD) is a general term for chronic inflammatory disorders of unknown cause involving the gastrointestinal tract.1,2 Chronic IBD can be divided into two major groups chronic non-specific ulcerative colitis (UC) and Crohn's disease (CD). The causes include familial/genetic, infectious, immunological and psychological factors. An increased incidence of CD in monozygotic twins is strong evidence for a genetic component. The chronic inflammatory nature of these diseases has prompted a continuing search for infectious causes.1,2 Immune complexes too have been invoked to explain extraintestinal manifestations of IBD.3 Neurotransmitter changes could modulate the predisposition to IBD. Geschwind has postulated a relationship between cerebral lateralization, immune function and systemic disorders. For example, they observed a higher frequency of left-handedness in patients with some immune disorders.4 There are no reports on the role of hemispheric dominance in the pathogenesis of IBD. The isoprenoid pathway is a key regulatory pathway in the cell. It produces digoxin an endogenous membrane Na+-K+ ATPase inhibitor which can produce immune activation as well as regulate neurotransmitter transport.5-7 Membrane Na+-K+ ATPase inhibition can lead to immune activation by increasing the intracellular calcium. Increased levels of endogenous ouabain like compoinds have been reported in autoimmune disorders and in psychiatric disorders like bipolar mood disorders.8 Since immune activation and psychiatric predilection are noted in IBD it was considered pertinent to study the isoprenoid pathway and the related biochemical cascade in this disorder. As hypothalamic digoxin can modulate synaptic transmission of multiple neurotransmitter systems, the pathway was also assessed in individuals with differing hemispheric dominance to find out the role of hemispheric dominance in the pathogenesis of IBD. The activity of plasma HMG CoA reductase, serum magnesium, digoxin, dolichol and ubiquinone as well as RBC Na+-K+ATPase activity were measured in patients with IBD and individuals with differing hemispheric dominance. The tyrosine / tryptophan catabolic patterns, glycoconjugate metabolism, free radical metabolism and RBC membrane composition were also assessed. The results are presented in this paper. METHODS 4 sets of patients / normal population (age group 20-30 years) were chosen for the study 15 cases of ulcerative colitis, 15 cases of regional ileitis, 15 cases of age and sex matched bihemispheric dominant controls and 15 cases each of right hemispheric, left hemispheric and bihemispheric dominant individuals diagnosed by the dichotic listening test. None of the subjects was under medication at the time when the blood sample was collected. None of the patients were smokers (active or passive). Informed consent was obtained from all the individuals / patients. The permission of the ethics committee of the institute was obtained. A blood sample in fasting state was collected from each of the patients for various estimations. RBCs were separated within 1 hour of the collection of blood for the estimation of membrane Na+-K+ ATPase. Serum was used for the estimation of HMG CoA reductase activity. Plasma/serum was used for the estimation of the other parameters. All biochemicals used in this study were obtained from M/s Sigma Chemicals, USA. Activity of HMG CoA reductase of the plasma was determined using the method of Rao and Ramakrishnan by determining the ratio of HMG CoA to mevalonate.9 For the determination of the Na+-K+ ATPase activity of the erythrocyte membrane, the procedure described by Wallach and Kamat was used.10 Digoxin in the plasma was determined by the HPLC procedure described by Arun et al.11 For estimation of ubiquinone and dolichol in the plasma, the procedure described by Palmer et al was used.12 Magnesium in the plasma was estimated by atomic absorption spectrophotometry.13 Amino acids and neurotransmitters tryptophan, tyrosine, serotonin and catecholamines and lipid peroxidation products (MDA, conjugated dienes and hydroperoxides) and reduced glutathione were estimated by procedures described in the Methods of Biochemical Analysis.14 Quinolinic acid content of plasma was estimated by HPLC (C18 column micro Bondapak 4.6 x 150 mm), solvent system 0.01 M acetate buffer (pH 3.0) and methanol (6:4), flow rate 1.0 ml/minute and detection-UV 250 nm). Morphine, strychnine and nicotine were estimated by the method described by Arun et al.15 Details of the procedures used for the estimation of total and individual GAG, carbohydrate components of glycoproteins, activity of enzymes involved in the degradation of GAG (beta glucuronidase, beta N-acetyl hexosaminadase, hyaluronidase and cathepsin D), and activity of glycohydrolases (beta galactosidase, beta fucosidase and beta glucosidase), are described before.16 Cholesterol was estimated by using commercial kits supplied by Sigma chemicals, USA. Serum phospholipids and glycolipids were estimated by the procedures described in the Methods of Biochemical Analysis.14 Superoxide dismutase, catalase, glutathione peroxidase and glutathione reductase were estimated by the procedures described in the Methods of Enzymatic Analysis.17 Statistical analysis was done by `ANOVA'. RESULTS The activity of HMG CoA reductase and the concentration of digoxin and dolichol were increased in ulcerative colitis and regional ileitis. The concentration of serum ubiquinone, the activity of erythrocyte membrane Na+-K+ ATPase and serum magnesium were decreased in ulcerative colitis and regional ileitis (Table 1). The concentrations of serum tryptophan, quinolinic acid and serotonin were increased while those of tyrosine, dopamine and noradrenaline were decreased in ulcerative colitis and regional ileitis. Nicotine and strychnine were detected in the plasma of patients with ulcerative colitis and regional ileitis and were undetectable in control serum. Morphine was not detected in the plasma of ulcerative colitis and regional ileitis (Tables 2 and 3). The concentration of total glycosaminoglycans (GAG) increased in the serum of ulcerative colitis and regional ileitis patients. The concentration of hyaluronic acid (HA), heparan sulphate (HS), heparin (H), dermatan sulphate (DS) and chondroitin sulphates (ChS) was increased in ulcerative colitis and regional ileitis. The concentrations of total hexose, fucose and sialic acid were increased in the glycoproteins of the serum in ulcerative colitis and regional ileitis. The activity of GAG-degrading enzymes, beta glucuronidase, beta N-acetyl hexosaminidase, hyaluronidase, cathepsin-D, was increased in ulcerative colitis and regional ileitis when compared to the controls. The activity of beta galactosidase, beta fucosidase and beta glucosidase increased in ulcerative colitis and regional ileitis (Tables 4 and 5). The concentration of total GAG, hexose and fucose in the RBC membrane decreased significantly in ulcerative colitis and regional ileitis. The concentration of cholesterol increased and of phospholipids decreased in the RBC membrane in ulcerative colitis and regional ileitis and the cholesterol:phospholipid ratio in the RBC membrane increased significantly in ulcerative colitis and regional ileitis (Table 6). The activity of superoxide dismutase (SOD), catalase, glutathione reductase and glutathione peroxidase in the erythrocytes decreased significantly in ulcerative colitis and regional ileitis. In ulcerative colitis and regional ileitis the concentration of MDA, hydroperoxides, conjugated dienes and nitric oxide (NO) increased significantly. The concentration of glutathione decreased in ulcerative colitis and regional ileitis (Table 7). The results showed that HMG CoA reductase activity, serum digoxin and dolichol were increased and ubiquinone reduced in left-handed / right hemispheric dominant individuals. The results also showed that HMG CoA reductase activity, serum digoxin and dolichol were decreased and ubiquinone increased in right-handed / left hemispheric dominant individuals.The results showed that the concentration of tryptophan, quinolinic acid, serotonin, strychnine and nicotine was found to be higher in the plasma of left-handed / right hemispheric dominant individuals while that of tyrosine, dopamine, morphine and norepinephrine was lower. The results also showed that the concentration of tryptophan, quinolinic acid, serotonin, strychnine and nicotine was found to be lower in the plasma of right-handed / left hemispheric dominant individuals while that of tyrosine, dopamine, morphine and norepinephrine was higher (Tables 8, 9 and 10). DISCUSSION The results showed that HMG CoA reductase activity, serum digoxin and dolichol were increased in IBD while serum ubiquinone was reduced. Previous studies in this laboratory had demonstrated incorporation of 14C-acetate into the digoxin in a rat brain indicating that acetyl CoA is the precursor of digoxin biosynthesis in mammals also.18 The elevated HMG CoA reductase activity correlates well with elevated digoxin levels and reduced RBC membrane Na+-K+ ATPase activity. The increase in endogenous digoxin, a potent inhibitor of membrane Na+-K+ ATPase, can decrease the activity of this enzyme. The inhibition of Na+-K+ ATPase by digoxin is known to cause an increase in intracellular calcium resulting from increased Na+-Ca++ exchange, increased entry of calcium via the voltage gated calcium channel and increased release of calcium from intracellular endoplasmic reticulum calcium stores.19 This increase in intracellular calcium by displacing magnesium from its binding sites, causes a decrease in the functional availability of magnesium.19 This decrease in the availability of magnesium can cause decreased mitochondrial ATP formation which along with low magnesium can cause further inhibition of Na+-K+ ATPase, since the ATP-magnesium complex is the actual substrate for this reaction. Cytosolic free calcium is normally buffered by 2 mechanisms ATP-dependent calcium extrusion from the cell, and ATP-dependent sequestration of calcium within the endoplasmic reticulum. The magnesium-related mitochondrial dysfunction results in defective calcium extrusion from the cell. There is thus a progressive inhibition of the Na+-K+ATPase activity, first triggered by digoxin. Low intracellular magnesium and high intracellular calcium consequent to Na+-K+ ATPase inhibition appear to be crucial to the pathogenesis of IBD. Serum magnesium was found to be reduced in IBD. Increased intracellular calcium activates calcium-dependent calcineurin signal transduction pathway which can produce T cell and macrophage activation with secretion of interleukin-3, 4, 5, 6, 8 and TNF alpha (Tumour necrosis factor alpha).20,21 This can also explain the immune activation in IBD. Increased concentration of mucosal IgG cells and changes in subsets of T cells, suggesting antigenic stimulation have been described in IBD.3 Activation of mucosal immune cells results in complex expression of cytokines, which may contribute to the mucosal inflammatory response.3 Membrane Na+-K+ ATPase inhibition can produce immune activation and is reported to increase CD4/CD8 ratios as exemplified by the action of lithium. Digoxin, apart from affecting cation transport is also reported to influence the transport of various metabolites across cellular membranes, including aminoacids and various neurotransmitters.7 The results showed that the concentration of tryptophan, quinolinic acid and serotonin was found to be higher in the plasma of patients with IBD while that of tyrosine, dopamine and norepinephrine was lower. Thus there is an increase in tryptophan and its catabolites and a reduction in tyrosine and its catabolites in the serum of IBD patients. This could be due to the fact that digoxin can regulate neutral aminoacid transport system with preferential promotion of tryptophan transport over tyrosine.7 The decrease in membrane Na+-K+ ATPase activity in IBD could be due to the fact that the hyperpolarising neurotransmitters (dopamine, noradrenaline and morphine) are reduced and the depolarising neuroactive compounds (serotonin, quinolinic acid, strychnine and nicotine) are increased. Quinolinic acid has been implicated in immune activation in other immune diseases like lupus and could contribute to the same in IBD.22 Serotonin, dopamine and noradrenaline receptors have been demonstrated in the lymphocytes. It has been reported that during immune activation serotonin is increased with the corresponding reduction in dopamine and noradrenaline in the brainstem monoaminergic nuclei.23 Thus, elevated serotonin and reduced noradrenaline and dopamine can contribute to the immune activation in IBD. We had already shown the presence of endogenous morphine in the brains of rats loaded with tyrosine, and endogenous strychnine and nicotine in the brains of rats loaded with tryptophan.15 Serum of patients with IBD showed the presence of strychnine and nicotine but morphine was absent. The absence of morphine in patients with IBD is also significant. Morphine can inhibit the inflammatory response and the absence of morphine could contribute to an exaggeration of this response.24 The Schizoid neurotransmitter pattern of reduced dopamine, noradrenaline and morphine and increased serotonin, strychnine and nicotine is also noticed in IBD and could predispose to its development.25 Quinolinic acid, an NMDA agonist can contribute to NMDA excitotoxicity reported in schizophreniform psychosis. Strychnine, by blocking glycinergic transmission, can contribute to the decreased inhibitory transmission in schizophreniform psychosis. Recent data suggest that the initial abnormality in schizophreniform psychosis involves a hypodopaminergic state and the low dopamine levels now observed agree with this. Nicotine, by interacting with nicotinic receptors, can facilitate the release of dopamine, promoting the dopaminergic transmission in the brain. This can explain the increased dopaminergic transmission in the presence of decreased dopamine levels. The increased serotoninergic activity and reduced noradrenergic outflow from locus coeruleus reported earlier in schizophreniform psychosis, agree with our finding of elevated serotonin and reduced noradrenaline levels. A schizoid neurotransmitter pattern and personality can predispose to IBD. It has been reported that patients with IBD have a characteristic personality that renders them susceptible to emotional stresses.1,2 The low magnesium levels consequent to membrane Na+-K+ ATPase inhibition can affect the metabolism of GAG, glycoproteins and glycolipids.16 The elevation in the level of dolichol consequent to its increased synthesis, increases its availability of N-glycosylation of proteins. In magnesium deficiency, the glycolysis, citric acid cycle and oxidative phosphorylation are blocked and more glucose-6-phosphate is channelled for the synthesis of GAG. The results showed an increase in the concentration of serum total GAG, and carbohydrate components of glycoproteins (hexose, fucose and sialic acid) in IBD. The increase in the carbohydrate components of serum glycoproteins total hexose, fucose and sialic acid was not to the same extent in IBD, suggesting a qualitative change in glycoprotein structure. In IBD the percentage change in total hexose, fucose and sialic acid when compared to control is 54.3%, 20% and 33% respectively. The concentrations of hyaluronic acid, heparan sulphate, heparin, dermatan sulphate and chondroitin sulphates were increased in the serum of IBD patients. The activity of GAG-degrading enzymes and glycohydrolases was increased in the serum of IBD patients. The increase in the activity of glycohydrolases and GAG-degrading enzymes could be due to reduced lysosomal stability and consequent leakage of lysosomal enzymes into the serum. The increase in the concentration of the carbohydrate components of glycoproteins and GAG in spite of increased activity of many glycohydrolases may be due to their possible resistance to cleavage by glycohydrolases consequent to the qualitative change in their structure. A number of fructose and sialic acid containing natural ligands are involved in the trafficking of leukocytes, adhesion of the lymphocyte producing leukocyte trafficking and extravasation in to the perivascular space. The same immune phenomenon has been described in IBD.26 The protein processing defect can result in defective glycosylation of endogenous colonic glycoprotein antigens and exogenous bacterial glycoprotein antigens with consequent defective formation of MHC-antigen complex.27 The MHC-linked peptide transporter, a P-glycoprotein which transports MHC-antigen complex to the antigen presenting cell surface, has an ATP binding site which is dysfunctional in the presence of magnesium deficiency. This results in defective transport of MHC class 1 colonic glycoprotein antigen complex to the antigen presenting cell surface for recognition by the CD4 or CD8 cell. Defective presentation of endogenous colonic glycoprotein antigen can explain the immune dysregulation in IBD. This can contribute towards the autoimmunity in IBD. Patients with IBD have humoral antibodies to the colonic cells.3 In general, the presence and titer of these antibodies do not correlate with disease activity. Immune complexes have also been involved to explain extraintestinal manifestations of IBD. Altered glycoconjugate synthesis can lead to the generation of new endogenous colonic antigens, setting up an autoimmune process. Defective presentation of exogenous bacterial glycoprotein antigens can produce immune evasion by the bacteria and bacterial persistence. Persistent bacterial infections have been implicated in the pathogenesis of IBD. In patients with IBD there are reports of the isolates of cell wall variants of Pseudomonas.1,2 The chronic inflammatory nature of these diseases has prompted a continuing search for infectious causes. The alteration in the isoprenoid pathway specifically, cholesterol, as well as changes in glycoproteins and GAG can affect cellular membranes. The upregulation of the isoprenoid pathway can lead to increased cholesterol synthesis and magnesium deficiency can inhibit phospholipid synthesis. Phospholipid degradation is increased owing to an increase in intracellular calcium activating phospholipase A2 and D. The membrane composition was assessed by RBC membrane cholesterol: phospholipid ratio, carbohydrate residues of glycoproteins and total GAG. The cholesterol: phospholipid ratio of the RBC membrane was increased in IBD. The concentration of total GAG, hexose and fucose of glycoproteins, and cholesterol decreased in the RBC membrane and increased in the serum, suggesting their reduced incorporation into the membrane and defective membrane formation. The glycoproteins, GAG and glycolipids of the cellular membrane are formed in the endoplasmic reticulum, which is then budded off as a vesicle, which fuses with the golgi complex. The glycoconjugates are then transported via the golgi channel and the golgi vesicle fuses with the cell membrane. This trafficking depends upon GTPases and lipid kinases which are crucially dependent on magnesium and are defective in magnesium deficiency.28 The change in the membrane structure produced by alteration in the glycoconjugates and the cholesterol: phospholipid ratio can produce changes in the configuration of Na+-K+ ATPase resulting in further membrane Na+-K+ ATPase inhibition. The same changes can affect the structure of organelle membrane. This results in defective lysosomal stability and leakage of glycohydrolases and GAG-degrading enzymes into the serum. Lysosomal stability is important in the genesis of IBD as lysosomal enzymes can contribute to tissue destruction. The concentration of ubiquinone decreased significantly in IBD which may be the result of low tyrosine levels, reported in IBD consequent to digoxin's effect in preferentially promoting tryptophan transport over tyrosine.7 The aromatic ring portion of ubiquinone is derived from the tyrosine. Ubquinone is an important component of the mitochondrial electron transport chain and also contributes to free radical scavenging. The increase in intracellular calcium can open the mitochondrial PT pore causing a collapse of the hydrogen gradient across the inner membrane and uncoupling of the respiratory chain.29 Intracellular magnesium deficiency can lead to a defect in the function of ATP synthase. All this leads to a defect in mitochondrial oxidative phosphorylation, incomplete reduction of oxygen and generation of superoxide ion, which produces lipid peroxidation. The increase in intracellular calcium may lead to increased generation of NO by inducing the enzyme nitric oxide (NO) synthase which combines with superoxide radical to form peroxynitrite. Increased calcium can also activate phospholipase A2 resulting in increased generation of arachidonic acid which can undergo increased lipid peroxidation. Increased generation of free radicals like the superoxide ion, and the hydroxyl radical can produce lipid peroxidation and cell membrane damage, which can further inactivate Na+-K+ ATPase triggering the cycle of free radical generation again. There was an increase in lipid peroxidation as evidenced from the increase in the concentration of MDA, conjugated dienes, hydroperoxides and NO, with decreased antioxidant protection as indicated by the decrease in ubiquinone and reduced glutathione in IBD. Ubiquinone deficiency also leads to reduced free radical scavenging. The activity of the enzymes involved in free radical scavenging is decreased in IBD suggesting reduced free radical scavenging. The peroxisomal membrane is defective owing to the membrane Na+-K+ ATPase inhibition-related defect in membrane formation, and leads to reduced catalase activity. Magnesium deficiency can lead to inhibition of glutathione synthetase and glutathione reductase activity. Thus, the glutathione system of free radical scavenging is defective in the presence of membrane Na+-K+ ATPase inhibition. Superoxide dismutase exists in a mitochondrial and cytoplasmic form. Opening of the mitochondrial PT pore produces hyperosmolality and matrix expansion rupturing the outer membrane, resulting in loss of the mitochondrial dismutase and a decrease in its activity. The reduction in catalase, superoxide dismutase (SOD), glutathione peroxidase and glutathione reductase suggests reduced free radical protection. Mitochondrial dysfunction-related free radical generation has been implicated in the pathogenesis of the IBD. Free radicals can produce immune activation and contribute to the pathogenesis of IBD.1,2 Increased intracellular calcium activates phospholipase C beta which results in increased production of diacyglycerol (DAG) with resultant activation of protein kinase C.30 The protein kinase C (PKC) activates the MAP kinase cascade resulting in cellular proliferation. The decreased intracellular magnesium can produce dysfunction of GTPase activity of the alpha-subunit of G protein. This results in ras-oncogene activation, as more of the ras is bound to GTP rather than GDP. Phosphorylation mechanisms are required for the activation of the tumour suppressor gene P53. The activation of P53 is impaired owing to intracellular magnesium deficiency producing a phosphorylation defect.30 Upregulation of the isoprenoid pathway can result in an increased production of farnesyl phosphate which can farnesylate the ras-oncogene producing its activation. The ubiquitin system of catabolic processing of proteins is important in DNA repair mechanism. In case of intracellular magnesium deficiency, ubiquitin protein catabolic processing and DNA repair mechanisms are defective and this could contribute to oncogenesis. Thus there is increased tendency for neoplastic transformation in patients with IBD. There is also increased incidence of colonic carcinoma in patients with IBD.1 In left-handed / right hemispheric dominant individuals there was a derangement of the isoprenoid pathway. They had an upregulated HMG CoA reductase activity with increased digoxin and dolichol levels and reduced ubiquinone levels. The RBC membrane Na+-K+ ATPase activity was reduced and serum magnesium depleted. The left-handed/right hemispheric dominant individuals had increased levels of tryptophan, serotonin, quinolinic acid, strychnine and nicotine while the levels of tyrosine, dopamine, noradrenaline and morphine were lower. Thus an upregulated isoprenoid pathway, increased level of tryptophan and its catabolites, decreased levels of tyrosine and its catabolites and hyperdigoxinaemia are suggestive of right hemispheric dominance. In right-handed / left hemispheric dominant individuals these biochemical patterns were reversed. IBD occurs in right hemispheric dominant individuals and is a reflection of altered brain function. REFERENCES
Copyright 2003 - Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03048t1.jpg] [is03048t6.jpg] [is03048t10.jpg] [is03048t5.jpg] [is03048t9.jpg] [is03048t3.jpg] [is03048t4.jpg] [is03048t7.jpg] [is03048t8.jpg] [is03048t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}