 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 65, No. 3, May-June, 2003, pp. 260-262 Functional recovery in ureteropelvic junction obstruction after surgery A. W. Abrar, B. Singh, S. Mushtaq,* S. Khan,* A. Ahad, S. Yasin, R. Wani Departments of Urology and *Nuclear Medicine
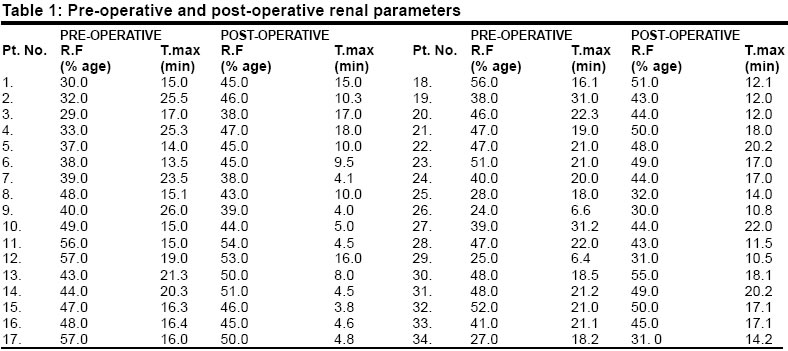
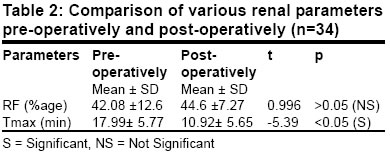
Paper Received: October 2002. Paper Accepted: January 2003. Source of Support: Nil Code Number: is03049 ABSTRACT A non-invasive test of renal function, renal scintigraphy using Tc99m DTPA was used to assess improvement of renal function in patients of ureteropelvic junction obstruction, after pyeloplasty. The study revealed that improvement in renal function occurred in 26.4 % of the patients while Tmax improved in 85.29 % of patients, revealing the fact that despite improvement in drainage, many kidneys fail to improve in function after pyelopasty. KEY WORDS: Renal function, Pyeloplasty, Renal scan. How to cite this article: Abrar AW, Singh B, Mushtaq S, Khan S, Ahad A, Yasin S, Wani R. Functional recovery in ureteropelvic junction obstruction after surgery. Indian J Surg 2003;65:260-62. INTRODUCTION Obstruction in the urinary tract affects all renal functional parameters depending on the pressure gradient across the obstructed site which affects the intrapelvic pressure.1 The decrease in renal function over time can be easily demonstrated by serial measurement of renal uptake and relative function (R.F.) using Tc99m DTPA scintigraphy. When intratubular luminal pressure increases in nephrons, there is increased reabsorption of salt and water and this leads to reduction in the flow of of non-reabsorabable solutes like Tc 99m DTPA through the nephrons.2 This leads to prolongation of Tmax (time required for maximum activity). The present study will analyze the effect of pyeloplasty on these parameters in patients with ureteropelvic junction obstruction. MATERIAL AND METHODS The study comprised 34 patients [24 men, with mean age of 24.53 years (range 12-45) and 10 women with mena age 23.21 years (range 13-40)]. All patients were having ureteropelvic junction obstruction as diagnosed on intravenous urogram (IVU). Ultrasonography was done in all the patients to exclude any associated anomaly. Patients were taken for surgery if they had significant decrease in relative function (d" 7% of normal) or Tmax was more than 5 minutes or if patients were symptomatic and were having radiographic evidence of ureteropelvic junction obstruction. Patients having bilateral obstructive uropathy, unilateral kidney, and associated calculi were excluded from the study. All the patients underwent renal scintigraphic study preoperatively and 12 weeks postoperatively. The scans were done using technetium 99m diethylenctriamine pentacetic acid (Tc99m DTPA) and were acquired on gamma camera Orbitor 75 (Siemens) interfaced to a computer icon (Siemens). An informed written consent was obtained from all the patients and permission from the institution's ethical committee was obtained. All patients were given 1 litre of water orally one hour before the study. Prior to intravenous administering of the radiopharmaceutical, the dose was calibrated in a dose calibrator [Capinitec, CRC -300 (USA)] after selecting the technetium window. The patients were placed in supine position with gamma camera detector underneath. An intravenous bolus dose of 185 MBq (5mci) was administered in antecubital vein, followed by saline flush. Post-injection activity of the syringe was measured and recorded. Phase I of the study included 60 frames of 1-second duration on a matrix size of 64x64, followed without a pause by Phase II, which included 60 frames of 30 seconds duration each. The patients were administered intravenous Lasix (0.5mg/kg body weight) at the 25th frame of Phase II. A pre-void static image of 2 minutes duration on a matrix size of 256x256 was acquired. After the completion of the pre-void image, the patients were made ambulatory and asked to void. A post-void static image of 2 minutes duration was acquired. The Phase I and Phase II images were processed on a computer using a predefined renal programme. The region of interest (R.O.I) around the kidneys was marked and from the computer relative function and Tmax were calculated. The values of both RF and Tmax were compared before and after pyeloplasty (Table 1). The mean and standard deviation was calculated, then the paired samples test (t-test) was used to compare the data obtained. From this p value was calculated at 95% confidence interval and hence p<0.05 was considered significant. RESULTS The mean RF was pre-operatively 42.08 ±12.6, which changed to 44.6 ± 7.27 (p>0.05) after pyeloplasty (Table 2). Overall, 9 patients (26.47%) showed improvement in RF while 25 (73.25%) failed to show significant improvement. The mean Tmax was preoperatively 17.99 ± 5.77, which got reduced to 10.92 ± 5.65 (p<0.05) after pyeloplasty and overall 29 patients (85.29%) showed decrease in Tmax after pyeloplasty. DISCUSSION In the management of obstructive uropathy one important aspect is to study various renal functional parameters which can be followed up later so as to assess the effect of obstruction on renal function and the recoverability of these after relief of obstruction. For this purpose, renography using Tc99m DTPA is an investigation of choice.3 In our study we studied relative function and Tmax in patients with radiologically diagnosed ureteropelvic junction obstruction, both preoperatively and post-operatively. Relative function implies what percentage of global renal function the kidney under evaluation contributes. Normal value of it is 42 to 58 since an error of 5-7% can occur in its evaluation; so when change occurred is >7% it is considered significant change. The recommended method for determining relative function comprises integration of the background subtracted renograms over 2-3 minutes for Tc99m DTPA.4 Individual renal function is then expressed in percentage terms on the ratio of the mean uptake for each kidney to the sum of the two. As obstruction proceeds, function is depressed and relative function reduced. When the patient is asymptomatic and relative function is normal conservative therapy carries no additional risk.5 Various studies revealed that pyeloplasty did not result in significant increase in renal function irrespective of the age of the patient, but such surgery may prevent further deterioration of function.6,7 The present study revealed that RF improved in 26.47% of patients and mean RF showed an insignificant improvement (p<0.05). Along with RF, we analyzed the effect of pyeloplasty on transit time of radioisotope across the kidney i.e., Tmax (time required for maximum activity). It is documented that continuing glomerular filtration with resistance to outflow increases intratubular pressure in nephrons, leading to increased re-absorption of salt and water. This leads to slowing of the flow of non-solutes through the nephrons and this further leads to prolonged transit time.2 In our study it showed a significant improvement post- operatively (p<0.05) and this improvement was seen in 85.29% of patients. These findings are quite consistent with those obtained by other authors.3,6 CONCLUSION Radionuclide renal scan is an effective, easy to perform, reproducible and objective technique to investigate various functional renal parameters in obstructive uropathy before and after intervention. Patients with ureteropelvic junction obstruction do not show an impressive change after pyeloplasty as evident by an insignificant change in RF. So if an asymptomatic patient has normal RF, he may be followed up by serial renal scans and in patients with abnormal RF, it may prevent further deterioration in function, as pyeloplasty led to an improvement in the drainage of kidneys in 85.29% patients and this was a statistically significant improvement. REFERENCES
Copyright 2003 - Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03049t1.jpg] [is03049t2.jpg] |
| |||||||||

{kind=link}
{kind=link}