 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 65, No. 3, May-June, 2003, pp. 263-268 Options in the management of solid visceral injuries from blunt abdominal trauma Srikant Mohapatra, Siba Prashad Pattanayak, K. Raja Ram Mohan Rao, Balakrishna Bastia* Departments of Surgery and *Radiodiagnosis, M.K.C.G. Medical College and Hospital, Berhampur 760004, Orissa, India.
Paper Received: March 2002. Paper Accepted: December 2003. Source of Support: Nil Code Number: is03050 ABSTRACT Non-operative management of solid visceral injuries from blunt abdominal trauma, especially in stable patients, has become the order of the day in developed countries. However, the safety and feasibility of such an approach in the absence of modern amenities like CT, angiography and ICU support has remained a point of controversy. This prospective study analyzes the manifestations, management and outcome of solid visceral injuries in 72 patients with blunt abdominal trauma, relying solely on readily available diagnostic modalities, viz. abdominal X-ray, ultrasonography and paracentesis, in the setting of a hospital lacking CT and ICU support. Road traffic accident was the most common mechanism of blunt abdominal trauma in our study, most victims being males in the third decade of life. Chest injury was the predominant associated injury (26%), but head injury was the most common extra-abdominal injury causing death. Plain abdominal X-ray accurately diagnosed all 3 cases of intestinal injury. Abdominal ultrasonography had a sensitivity of 89%, specificity of 100%, and accuracy of 100% in diagnosing abdominal solid visceral injuries. The sensitivity, specificity and accuracy of diagnostic paracentesis in detecting hemoperitoneum, were 82%, 86% and 90% respectively. 39% patients were ultimately subjected to laparotomy. Frequency of solid visceral injuries encountered were: liver 47.9%, spleen 29.2%, kidneys 14.6% and pancreas 8.3%. Organ salvage was possible in 90.3% of operated cases. Postoperative morbidity was 26%, mostly due to chest and wound infections. Non-operative morbidity rate was 20% with failure of non-operative management occurring in 10% cases. The overall mortality was 21%. All deaths in the non-operative group (mortality 9%) were due to associated head injury, whereas deaths in the operative group (14% mortality) were a consequence of the abdominal trauma and/or surgery. The average number of blood transfusions received by patients in the non-operative and operative groups were 0.5 and 3.0 respectively. The average duration of hospital stay was 7.8 days for the non-operative group and 10.4 days for the operative group. Thus, a multipronged approach employing abdominal X-ray, ultrasonography and diagnostic paracentesis, correlated with clinical findings, can be fairly useful and accurate in early diagnosis and management of solid visceral injuries from blunt abdominal trauma at a limited-resource set-up lacking CT and ICU support, with acceptable morbidity and mortality. KEY WORDS: Solid visceral injury, Blunt abdominal trauma, Management. How to cite this article: Mohapatra S, Pattanayak SP, Rao KRRM, Bastia B. Options in the management of solid visceral injuries from blunt abdominal trauma. Indian J Surg 2003;65:263-8. INTRODUCTION Blunt Abdominal Trauma (BAT) has often proved to be the trauma surgeon's nemesis, due to the multitude of its manifestations. The recent trend is heavily in favour of non-operative or conservative surgical management of abdominal solid visceral injuries given the various sophisticated and highly accurate non-invasive imaging tools at the trauma surgeon's disposal today. However, the feasibility and safety of such an approach, especially in a limited-resource set-up, hamstrung by the non-availability of ICU and advanced imaging/interventional techniques like CT and angiography, has often been a contentious issue. This prospective study was undertaken to evaluate the pattern of solid visceral injury (SVI) arising from BAT with special reference to its management and outcome in the setting of a hospital lacking surgical ICU and CT support. The results were considered vis-à-vis data from other studies. MATERIAL AND METHODS Eighty-one cases of BAT were admitted to the surgical wards over a 24-month period (April 1999 to March 2001) of whom 9 expired before any medical intervention could be done. The rest of the 72 salvageable cases were included in the present study. Patients from all age groups and both sexes were considered. Those patients declared dead before primary medical intervention, referred elsewhere or lost to evaluation were excluded from the study, as were patients with combined blunt and penetrating mechanisms of abdominal trauma and those with associated systemic illnesses complicating the clinical picture. On admission, all patients were resuscitated with IV fluids/blood transfusion and advised bedrest with haemodynamic monitoring at hourly intervals. Serial haematocrit, haemoglobin estimation, blood grouping and cross-matching and other appropriate laboratory investigations were performed. Appropriate antibiotic therapy and tetanus prophylaxis was also instituted. All patients were subjected to straight X-ray abdomen followed by 4-quadrant wide-bore needle (16 G) diagnostic abdominal paracentesis (DPC) as screening procedures. All underwent abdominal Ultrasonography (USG) [Wipro GE 9T 3200 Advantage II], initially F.A.S.T. (Focused Abdominal Sonography for Trauma) and whenever the condition permitted, a detailed sonological evaluation followed, with independent opinion from the consultant sonologist. Alert and haemodynamically stable patients (as indicated by normal vital signs, urine output of 30-50 ml/hr and minimal blood product requirement) without any signs of peritoneal irritation on repeated abdominal examination, and with normal findings on radiological and sonological evaluation, were chosen for initial non-operative management. A decision for laparotomy was taken based on one or more of the following criteria:
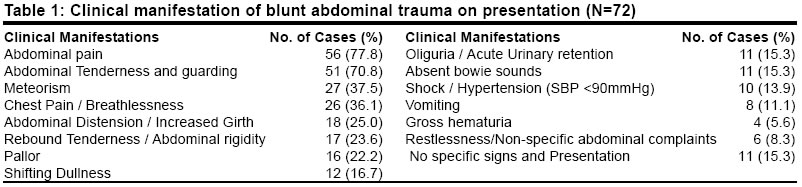
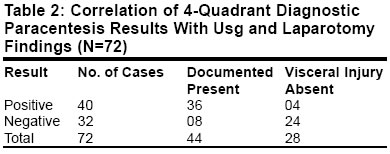
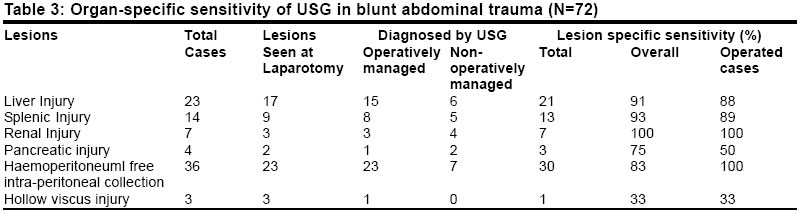
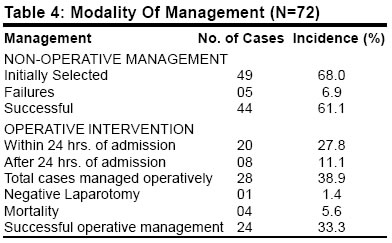
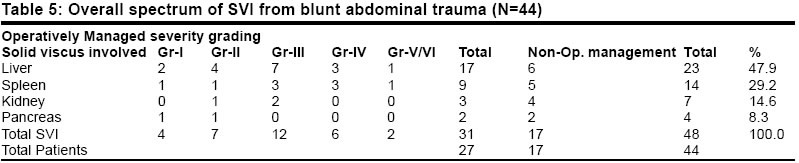
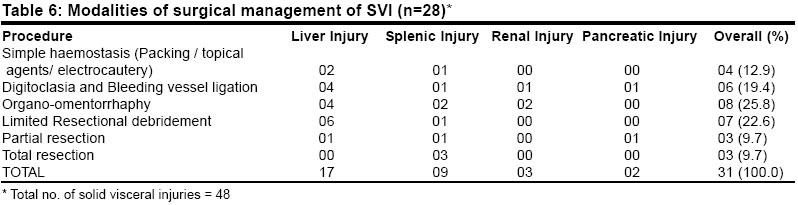
Urgent laparotomy without waiting for detailed investigations was mandated by the presence of abdominal distension and hypotension, overt peritonitis or obvious signs of abdominal visceral injury. Intraoperatively the solid visceral injuries were graded as per the organ injury scale laid down by the American Association for the Surgery of Trauma.1 Options in operative management included simple haemostatic measures (viz. packing, surgicel / gel foam, electrocauterization), digitoclasia and individual bleeding vessel ligation, organo-omentorrhaphy, limited resectional debridement, partial resection and total resection. The outcome was assessed in terms of immediate morbidity and mortality, and findings on follow-up over the next 1-3 years. RESULTS Blunt trauma was the major mechanism of abdominal injury comprising 44% of our inpatients with abdominal trauma. In addition, 17% had combined blunt and penetrating mechanisms of injury (excluded from our study). More than 3/4th of the victims were in the first 4 decades of their lives, with the majority (33.3%) belonging to the 21-30 years age group. Male-Female ratio was 7:1. Road traffic accidents (RTA) were the most common aetiology (62%) mostly involving pedestrians or two wheeler riders (combined, 47%). 22% victims were found to be intoxicated at the time of the mishap. Chest injury was the most common associated extra-abdominal injury (26%) followed by head injury and other bony injuries (21% each). The most common symptom of BAT was abdominal pain (77.8%) (Table 1). Surprisingly, a sizeable proportion of cases presented with predominant chest complaints (36.1%). 8% patients presented with non-specific / minimal abdominal complaints, 2 of whom subsequently required surgical intervention for pancreatic trauma. Abdominal tenderness and guarding were the most common signs (70.8%) of BAT. 13.9% had hypotension on admission. Again, clinical findings were equivocal in 15.3% patients at presentation, of whom 2 presented late with pancreatic injury requiring operation. Physical findings proved to be misleading in 18% of patients in whom they were equivocal. No particular laboratory investigation was specific for SVI in BAT (Table 1). Abdominal X-ray was inconclusive in 64% of cases, but accurately diagnosed all 3 cases of hollow visceral injury. Four-quadrant DPC had a sensitivity of 82%, specificity of 86% and diagnostic accuracy of 90%, in detecting hemoperitoneum (Table 2). Abdominal USG was 100% accurate and specific in diagnosing abdominal SVI with a sensitivity of 89%, 7% false negative results and no false positive results overall, when correlated with laparotomy findings. However, it was inconclusive in 28% cases of BAT. It was most sensitive for renal injuries (100%) and least so for hollow visceral injury (33%). Average organ-specific sensitivity of abdominal USG was 80% (Table 3). Based on the aforementioned criteria for surgical triage, 49 patients (68%) were initially chosen for non-operative management with 5 (7%) failures (converted to laparotomy). 39% patients were ultimately subjected to laparotomy with 1 proving to be non-therapeutic (Table 4). Forty-four patients had documented solid visceral injuries (sonologically or at laparotomy). Overall, the liver was the most frequently injured solid organ (47.9%) in BAT followed by spleen (29.2%), kidney (14.6%) and pancreas (8.3%). Grade III injuries predominated at laparotomy (38.7%), with the proportion of major injuries (Grade III) higher for spleen (78%) than for liver (65%) (Table 5). Concomitant hollow visceral injury was infrequent in BAT (4%). Electrocautery and surgicel pack were the most common haemostatic methods employed, especially for minor (Grade II) injuries. Organ salvage was successful in 90.3% of cases operated. Only 1 patient succumbed to haemorrhagic shock intraoperatively from extensive hepatic injury, and total resection was necessitated in 3 cases of major splenic trauma (Table 6). Infection prevailed as the most common cause of postoperative morbidity (26%), predominantly wound and chest infections. Other complications were peritonitis and intraabdominal abscess, secondary haemorrhage, septicaemia and fistula formation. The overall postoperative morbidity rate was 29% (8 patients). The total number of patients developing various complications in the non-operative group was 10, with a morbidity rate of 20%. This included failure of non-operative management: due to uncontrolled secondary haemorrhage (2 cases), missed pancreatic injuries (2 cases) and delayed splenic rupture (1 case). Other complications were due to intraabdominal or chest infections. Mortality was 14% in the operative group and 9% in the non-operative group with an overall mortality of 21% from BAT. All deaths in the non-operative group were due to associated cranio-cerebral trauma, whereas haemorrhagic shock, septicaemia, uraemia and anaesthetic complications equally contributed to the deaths in the operative group. The average number of blood transfusions received by patients in the operative group was 3 units and for those in the non-operative group, it was 0.5 units. The average duration of hospital stay was 7.8 days for the non-operative group and 10.4 days for the operative group. Only 46 patients could be followed up for > 1 year (8 deaths, 18 lost to follow-up). Of them, 24% had some delayed complication, viz. incisional hernia, symptoms due to bands and adhesions, recurrent urinary tract infection, chronic discharging sinuses or pyrexia of unknown origin. The remaining 76% had an uneventful recovery. DISCUSSION Patients admitted with clinical suspicion of BAT are actually proved to have definite intraabdominal injuries in only about one-third cases. On the other hand, the abdomen epitomizes the problem of missed injuries, with significant findings being absent in 23-36% of patients with intraabdominal injuries.2 A missed splenic injury is the most common cause of preventable death in BAT patients.3 40% of patients with significant haemoperitoneum have no peritoneal signs.4 The masking effect of concurrent extra-abdominal injuries and altered sensorium from hypovolaemic shock, head injury or alcohol intoxication further compound the problem.5,6,13 The propensity for low pressure bleeding from solid viscera often makes it difficult to predict which injuries are likely to be self-limiting solely from initial clinical findings.4 The role of CT in the early diagnosis and management of BAT has often been overemphasized. Though it remains one of the most precise diagnostic tools for assessment of severity and follow-up of SVI, its ability to serve as a primary triage tool has been strongly challenged.5 It is time-consuming, expensive, needs specially trained operating personnel, misses hollow visceral injuries and some retroperitoneal lesions in an acute setting, and often lacks round-the-clock accessibility at most centres.2 USG, on the other hand, is safer (especially in paediatric and pregnant patients), simpler to perform, relatively cost-effective, rapidly confirms significant haemoperitoneum and simultaneously evaluates the thorax and retrope ritoneium in addition to the abdomen.2,5 Abdominal USG is now the method of choice for rapid evaluation of the abdomen for blood in unstable patients.3,9 A recent trial by Boulanger et al10 in 1999 revealed that a USG (FAST)-based algorithm for BAT was more rapid, less expensive and as accurate as an algorithm that employed CT or DPL instead.10 DPC has stood the test of time as a simple and fairly reliable bedside screening procedure for detection of significant haemoperitoneum, without being oversensitive like DPL.7,8 Used in conjunction with USG, it proved to be a useful diagnostic aid in our study, with an accuracy of 90% in detecting haemoperitoneum. The common presenting features of intraabdominal injury in most series are abdominal pain, tenderness, guarding and distension.8,11 Additionally, we noticed chest symptoms (chest pain / breathlessness) to be a surprisingly common association in more than one-third cases of BAT. Though hepatosplenic injuries still remain the most common SVI in BAT, liberal use of an advanced high resolution imaging technique like CT has revealed that the liver is the commonest solid organ injured in BAT and not the spleen as popularly believed.3,11 Our observations, though relying primarily on USG, are in agreement with this view. Almost three-fourths of SVI encountered at laparotomy were of grade I-III and isolated, which could have been managed non-operatively at well-equipped trauma centres. However, lack of ICU and CT support at our institution prompted us to tread cautiously and opt for laparotomy in case of doubt ("when in doubt it is better to open and see than to wait and watch"-Grey Turner). Over the past few decades, there has been an overwhelming trend in favour of non-operative management of SVI, irrespective of the grade of injury, especially for isolated organ injuries in younger, alert, haemodynamically stable patients, encouraged by the increasing availability and accuracy of various advanced imaging techniques for patient monitoring.3,12 This has resulted in a sharp decline in both therapeutic and non-therapeutic laparotomy rates. The laparotomy rate for BAT in most modern set-ups worldwide is only about 20% today.13 Whereas non-operative management carries the inherent risks of a missed hollow visceral injury, delayed bleeding, and risks associated with repeated transfusions, laparotomy carries a different set of risks that are primarily related to the surgeon, the anaesthesia, the nature of operation and its potential sequelae, and patient-related risk factors. The choice between the two modalities of management should be guided by haemodynamic considerations rather than the severity of organ injury.4 26% of all documented hepatic injuries in our study were managed non-operatively, the rest underwent conservative surgical management, with intra operative death in one case from excessive haemorrhage. 64% of splenic injuries required operation intervention with total splenectomy performed in 3 cases (21.4%). Organ salvage was possible in the rest of the 79.6% cases, including one case of delayed splenic rupture. A 100% renal salvage was possible in our study, though exploration rate was much higher (43%) compared to the less than 10% figure quoted elsewhere.14 This incongruence is due to the higher proportion of associated abdominal visceral injuries in our series. Of the 4 pancreatic injuries documented in the present study, 2 were explored late (> 24 hrs) after failure of non-operative management. One of them developed a pancreatico-cutaneous fistula and died of septicaemia and MODS. Infections prevail as the most common cause of morbidity in BAT. These ensue from the detrimental effects of hypovolemia, multiple blood transfusions, peritoneal soiling, and poor tisue handling at operation upon the physiological defence mechanism. In the Indian context, wide prevalence of malnutrition and unhygienic practices also contribute. The overall mortality from BAT was 21%. The early mortality rate was relatively high in our study (11%) mainly due to lack of pre-hospital resuscitation, and delay in transport of patients to the hospital, which prevented timely intervention in the "golden hour" of trauma. The postoperative mortality was higher compared to that in the non-operative group and was directly or indirectly attributable to the immediate intraabdominal injury. This was because the injuries mandating surgical intervention were generally of greater severity than those managed non-operatively and were more likely to be associated with polytrauma and/or haemodynamic instability. In contrast, abdomen-related mortality was nil in the non-operatively managed patients, with all deaths being the result of associated severe cranio-cerebral trauma. One patient with pancreatic trauma succumbed to septicaemia following laparotomy. CONCLUSION Blunt abdominal injuries pose a formidable diagnostic and therapeutic dilemma for the attending trauma surgeon, owing to their frequent occurrence as part of polytrauma, the wide range of visceral injuries that may result, the diversity of their presentations and the apparent lack of correlation between early physical findings and the severity of intraabdominal injury. Lately, the advent of sophisticated imaging technology has somewhat lightened the trauma surgeon's burden. In the absence of CT scan and other modern amenities, plain abdominal radiography, 4-quadrant DPC and abdominal USG can be put to good use as screening tools for surgical triage of patients with suspected solid visceral injury from BAT. These are readily available, rapid, safe, relatively inexpensive, minimally invasive, can be performed at the bedside (using mobile X-ray and USG units) and can predict SVI from BAT fairly accurately, especially when used in tandem. However, even today nothing surpasses the value of repeated clinical assessment by an experienced surgeon, in guiding the ultimate therapeutic decision. REFERENCES
Copyright 2003 - Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03050t4.jpg] [is03050t3.jpg] [is03050t5.jpg] [is03050t2.jpg] [is03050t1.jpg] [is03050t6.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}