 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
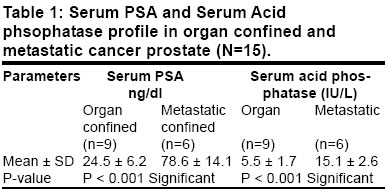
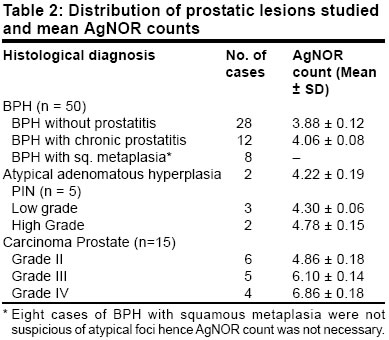
Indian Journal of Surgery, Vol. 65, No. 3, May-June, 2003, pp. 269-272 Diagnostic and prognostic significance of prostatic intraepithelial neoplasia in patients presenting with symptoms of prostatism R. C. Kesarwani, Ajay Kumar Gupta, Vipin Kumar Address for correspondence Dr. R. C. Kesarwani, Asso. Prof. of Surgery, Postgraduate Dept. of Surgery, M. L. N. Medical College and Associated SRN Hospital, Allahabad 211001. Paper Received: May 2002. Paper Accepted: January 2003. Source of Support: Nil Code Number: is03051 ABSTRACT A total of 70 patients with symptoms of prostate enlargement were studied and all of them were subjected to digital rectal examination, serum prostate specific antigen, serum acid phosphatase and ultrasonography. Prostatic tissue from transurethral resection 30 cases (43%), enucleation specimens 30 cases (43%), and transrectal tru-cut biopsy 10 cases (14 %), were obtained to ascertain the histological nature of the disease. It was found that 50 cases (71.4 %) were of benign prostatic hyperplasia, 15 (21.4 %) were prostatic carcinoma and the remaining 5 (7.1%) cases were prostatic intraepithelial neoplasia (PIN). Suspected cases were reviewed by haematoxylin and eosin staining and argyrophillic nucleolar organizer region (AgNOR)-staining and counting. In patients with benign lesions the mean AgNOR counts were between 3.5-4.5, in those with PIN the counts were between 4-5.5 and in those with carcinoma prostate the counts were higher than 5. AgNOR counting appears to be a good adjuvant to the existing diagnostic aids and provides better therapeutic and prognostic options for the clinicians. KEY WORDS: Prostatic intraepithelial neoplasia, Carcinoma prostate, AgNORs. How to cite this article: Kesarwani RC, Gupta AK, Kumar V. Diagnostic and prognostic significance of prostatic intraepithelial neoplasia in patients presenting with symptoms of prostatism. Indian J Surg 2003;65:269-72. INTRODUCTION Confronting patients, distressed and annoyed with symptoms of prostatism, has led clinicians to seek a pathological putative precursor lesion that could be diagnosed earlier in life. In 1987 Bostwick and Brawer1 proposed the term "Prostatic Intraepithelial Neoplasia" (PIN) fulfilling the majority of the requirements for a pre-malignant change in human prostate. PIN is considered the most likely precursor of clinically significant prostate cancer. Possibility of cure is highest at the stage of PIN. Tests carried out to identify the preclinical stages of prostate cancer include serum prostate specific antigen (PSA), digital rectal examination (DRE) and ultrasonography of prostate with or without guided biopsy. There is some available literature in which argyrophillic nucleolar organizer region (AgNOR)-staining in prostatic neoplasm and intraepithelial neoplasia were studied. This study stimulated us to include this AgNOR-staining technique in prostatic neoplasm to study the diagnostic and prognostic significance of PIN in patients presenting with symptoms of prostatism. MATERIAL AND METHODS A total of 70 cases were studied during a one-year period and all the cases were initially evaluated by history and physical examination. Following clinical diagnosis of BPH and carcinoma of prostate, further investigations to confirm the diagnosis of carcinoma were made utilising serum acid phosphatase value > 9 IU/L, SPSA value > 8 ng/dl. Ultrasonography of prostate showing hypoechogenecity and/ or with varing echogenecity was taken as Ca prostate. Criteria for organ-confined carcinoma of prostate included no capsular penetration, no seminal vesicle and no lymph node involvement. Histopathological examination of transrectal tru-cut needle biopsy, TUR or enucleated specimens of prostate were made and classified histologically as benign lesions, viz. BPH with or without prostatitis and atypical adenomatous hyperplasia. Premalignant lesions (PIN) were distributed according to McNeal (1986)2 and carcinoma prostate was graded according to Gleasons (1977)3 microscopic grading system. Slides were reviewed for area of atypical hyperplasia and foci of PIN. Slides of each suspected block were prepared from different planes for haematoxylin and eosin staining and for AgNOR staining and counting. To analyze, the AgNOR were counted in 100 nuclei in a random field under x 1000 magnification using x 100 oil emersion objective. AgNOR index was calculated as mean number of NORS per nucleus. Significance of AgNOR counts between benign and through various grades of malignant tumor cases were calculated using student `t' test. RESULTS In our study, obliteration of median groove (80%), hardness (80%) with nodularity (73%) emerged as the most effective predictor of prostate cancer on digital rectal examination (DRE). Mobility restriction and rectal mucosal involvement were seen in 25-35% of cases. In PIN, firm prostate was the predominant finding with nodularity seen in 20% of cases. Serum PSA and acid phosphatase values were within normal range in 70-90% cases of BPH and PIN. Serum PSA (normal value 0-4 ng/dl) in Ca prostate cases (n=15) was > 4 ng / dl in 86% cases, of which 70% had value > 12 ng / dl. Serum acid phosphatase was more than the normal range (0-9 IU/L) in 40% of cases. Mean serum PSA value in organ-confined (n=9) was 24.5 ± SD 6.2, whereas mean value of metastatic carcinoma prostate (n=6) was 78.6±SD14.1. Similarly, mean serum acid phosphatase value in organ-confined was 5.5±SD1.7, whereas in metastatic carcinoma prostate mean value was 15.1±SD2.6 (Table 1). In carcinoma of prostate, on USG, prostate was hypoechoic (53.3%), Isoechoic (13.1%) and with varying echogenecity in the rest of 33.3% cases. Similarly, PIN was hypoechoic in 60% and isoechoic in the remaining 40% cases. The mean AgNOR count of various prostatic lesions was noted. Mean AgNOR count of BPH without prostatitis (n=28) was 3.88 ± SD 0.12, whereas that of BPH with chronic prostatitis (n=12) was 4.06 ± SD 0.08. Group of atypical adenomatous hyperplasia (AAH) (n=2) had mean AgNOR count 4.22 ± SD 0.19. Mean AgNOR count of PIN (n=5) was 4.52 ± SD 0.20; when taken separately, low-grade PIN mean AgNOR count was 4.30 ± SD 0.06, high-grade had further increase in mean AgNOR count, and it was 4.78 ± SD 0.1 5. It was observed that mean AgNOR count increased with increasing grade of carcinoma prostate. Mean of grade II carcinoma prostate (n=6) was 4.86 ± SD 0.18, whereas that of grade III was 6.10 ± SD 0.14. Mean of grade IV carcinoma prostate was 6.86 ± SD 0.18 (Table 2). DISCUSSION On DRE of prostate, obliteration of the median groove, hardness and nodularity were the findings suggestive of carcinoma of prostate. Restriction of mucosal mobility (6.6%) with rectal mucosal involvement (33.3%) were suggestive of locally advanced cancer but 40% were not actually organ-confined. Partin et al observed that DRE tends to under-stage the diease.4 Patients with BPH had serum PSA and serum acid phosphatase values predominantly within the normal range. Increased serum PSA in PIN cases was not seen in our study or in the study by Ronnett.5 Level of serum PSA > 8 ng/dl, serum acid phosphatase > 9 IU/L came to be predictive of carcinoma prostate. Also, a statistically significant (p < 0.001) difference was seen in their mean values in organ-confined and metastatic cancer prostate. Hypoechoic prostate on USG was the feature suggestive of carcinoma prostate (53.3%) and PIN (60%), consistent with Lee et al (1986).6 The finding of isoechoic cancer was around 30-40% in recent American studies, but 13.3% in our study. The difference could be attributed to the use of trans-rectal ultrasonography by these investigators, which is superior to the trans-abdominal USG used in our study. In our present study the mean AgNOR count in benign lesions was in the range of 3-4, but significant increase (P < 0.001) in the mean AgNOR count of AAH was seen from BPH. It is evident from this study that the mean AgNOR count in PIN cases was significantly higher (P<0.001) than BPH cases, quite similar to that observed by Mukherjee,7 but there was no significant increase from AgNOR counts of AAH. This is due to the fact that AgNORs increase with increased mitotic activity (Wachtler, 1988),8 but Cheville (1990),9 failed to observe any change in the AgNORs of BPH and PIN. When taken separately, low-grade PIN mean AgNOR count shows significant increase (P<0.001) from BPH and a not-so-significant increase from AAH, thus implicating its benign tendency. Mean AP-NOR count of high-grade PIN shows significant (P < 0.001) increase from low-grade PIN count, in accordance with Mukherjee.7 This could be because high-grade PIN in comparison to low-grade PIN have much more nucleolar and nuclear abnormality (McNeal JE, 1986).6 Increase in AgNOR count from benign to various grades of carcinoma prostate in our study corroborated with Helpap B (1995)10 because of the fact described above. The increase in mean Ag-NOR count of grade II from high-grade PIN was not significant, but it was significant from high-grade PIN, BPH and AAH. This could be because high-grade PIN are quite similar to grade II carcinoma prostate at the cytological level in degree of cellular atypia. There is a good degree of concordance in the DNA ploidy pattern of both lesions (Barretton GB, 1994).11 A significant increase in the mean Ag-NOR count of grade III from grade II carcinoma prostate was seen, however, no significant increase in the mean Ag-NOR count from grade III to grade IV was observed, consistent with Contractor et al (1991).12 This is because changes in the distribution of the number and size of Ag-NORs reflect different arrangements of actively transcribing DNA without significant change in total volume.13 Thus, Ag-NOR count in our study was important in differentiating benign, pre-malignant and malignant prostatic lesions. CONCLUSION The use of Digital Rectal Examination, Ultrasound-guided biopsy with serum prostate specific antigen testing was found to be a better technique to detect prostate cancer early. When prostate biopsy specimen is reported to contain an atypical focus suspicious of prostate intraepithelial Neoplasia (PIN) or early malignancy, Ag-NOR counting can be used as a good adjuvant to other existing investigations in diagnosing these pre-malignant lesions (PIN) or early stage malignancy of which prognosis becomes better. REFERENCES
Copyright 2003 - Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03051t1.jpg] [is03051t2.jpg] |
| |||||||||

{kind=link}
{kind=link}