 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 65, No. 3, May-June, 2003, pp. 273-274 Case Report Successful surgical removal of Palmaz stent stuck in the left superficial femoral artery Masanori Fujita, Masafumi Shimizu, Hiroshi Yoshizu,* Susumu Tanaka, Tadaaki Maehara Department of Surgery II, National Defense Medical College, 3-2, Namiki, Tokorozawa,
Saitama, 359-8513, and *Hanno Clinic, 12-9, Higashi-cho, Hanno, Saitama, 357-0034,
Japan.
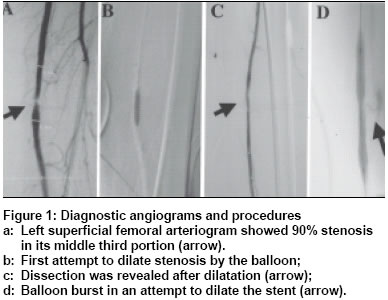
Paper Received: December 2002. Paper Accepted: December 2002. Source of Support: Nil Code Number: is03052 ABSTRACT This report describes a case of the successful surgical removal of a Palmaz stent accidentally stuck in the left superficial femoral artery. A 58-year-old man was referred to us with complaints of intermittent claudication in his left leg after walking 500 metres. Diagnostic angiography of the lower extremity showed 90% stenosis with a short segment at the left superficial femoral artery and percutaneous transluminal angioplasty (PTA) was performed. The angiogram just after PTA revealed a dissection of the artery. A Palmaz stent implant was attempted in order to seal off the dissection. The balloon used to dilate the stent burst, resulting in insufficient stent expansion, and it became stuck. Surgical operation to remove the stuck stent and reconstruct the blood flow through the left superficial femoral artery by artificial prosthesis grafting proved successful. KEY WORDS: Palmaz stent, Femoral artery, Complication, Surgical removal. How to cite this article: Fujita M, Shimizu M, Yoshizu H, Tanaka S, Maehara T. Successful surgical removal of Palmaz stent stuck in the left superficial femoral artery Indian J Surg 2003;65:273-4. INTRODUCTION Recently, endovascular stent placement for obstructive arterial disease is being increasingly employed.1 Accordingly, more complications during this procedure have been reported.2,3 With the improvements in new devices, the number of complications may increase.4 Once such complications occur, one must undertake reconstruction as soon as possible and do so less invasively. We report a case of the successful surgical removal of a Palmaz stent accidentally stuck in the left superficial femoral artery. CASE REPORT A 58-year-old man was referred to our outpatient clinic. His complaint was intermittent claudication in the left leg after walking 500 metres. Both his parents had suffered brain infarction. On examination, his blood pressure was 144/82 mmHg. On blood test, the total cholesterol level was 252 mg/dl and the serum triglyceride level was 337 mg/dl. Ankle brachial index (ABI) was 1.09 in the right leg, against 0.73 in the left. His electrocardiogram was normal. Diagnostic angiography of the lower extremity done with puncture of the right femoral artery showed 90% stenosis with short segment in the middle portion of the left superficial femoral artery (Figure 1a). During this procedure, intravenous heparin was injected. On the basis of the angiography findings, a decision to perform percutaneous transluminal angioplasty (PTA) was made. A five-French (5-Fr) crossover sheath was introduced via the right femoral artery. On the first attempt, the left superficial femoral artery stenosis was dilated with an angioplasty balloon 5-mm in diameter, 2-cm long and another balloon 5-mm in diameter and 4-cm long (Figure 1b). The post-angioplasty angiogram revealed a dissection of the artery (Figure 1c). A Palmaz stent 5-mm in diameter and 3-cm long was then implanted via the right femoral artery to seal off the dissection. The stent was also delivered to the right place and to implant it firmly, the balloon was dilated inside the stent. The balloon used to dilate the stent ruptured. The dye stored inside leaked into the branched artery, and the stent became stuck in the left superficial femoral artery. The balloon catheter burst, resulting in insufficient stent expansion and it became stuck. (Figure 1d). With a left femoral antegrade approach, a 5-Fr sheath was placed and another balloon was inserted to dilate the stent again but this manoeuvre failed. Surgical operation was performed to remove the stuck stent and to reconstruct the blood flow. The left superficial femoral artery was exposed as far as the portion just proximal to the popliteal artery between the sartorius muscle and the medialis muscle. The stuck stent and dilated balloon were removed in situ, the guide wire was cut off in the proximal portion, then removed via the right femoral artery. The proximal portion of the left superficial femoral artery was ligated. A left common, femoral artery to popliteal artery bypass was then performed using ringed GORE-TEX 6-mm in diameter. The proximal anastomosis was end-to-side and the distal one an end-to-end using two-armed continuous suture technique using 5-0 monofilament polypropylene. In the ruptured balloon, a pinhole was found near the proximal edge of the stent. The body of the stent was too twisted to expand. Improper handling at the initial insertion might have caused the twist. The follow-up angiography on the 14th postoperative day showed sufficient flow through the prosthesis (Figure 2). The ABI of the left lower extremity improved to 1.0 from 0.73. The patient received warfarin potassium from the 3rd postoperative day and this was continued later. DISCUSSION Intravascular stenting of the iliac artery or an artery in an extremity is a relatively safe and minimally invasive therapy for arterial occlusive disease. But the rare cases reported with complications in the procedure include bursting of an expanding balloon or wedging as a result.2,3 Though a percutaneous evacuation device for complications during Palmaz stent placement was available, in our case the stent expanded improperly and the balloon burst and became stuck in situ together with the stent. This may result in even further undesirable complications such as extended distal thrombosis.5 Further, percutaneous manipulations for evacuation might cause damage or destruction of the artery in situ. Thus, we had to perform surgical retrieval as soon as possible. Stenting in an extremity artery is extremely effective for older or high-risk cases. Complications during the procedure are very few, but surgical intervention is often needed. We believe that cases requiring surgical may be on the increase and therefore back-up from a surgical should be considered while undertaking vascular interventional procedures. REFERENCES
Copyright 2003 - Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03052f1.jpg] [is03052f2.jpg] |
| |||||||||

{kind=link}
{kind=link}