 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 65, No. 3, May-June, 2003, pp. 275-276 Case report Cystic replacement of kidney mimicking ascites Yousuf Perwez, Harprit Singh, Pramod Kumar Gondal Department of Surgery, Tata Main Hospital, TISCO, Jamshedpur 831005, Jharkhand.
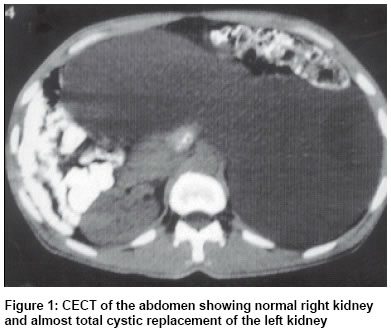
Paper Received: May 2001. Paper Accepted: September 2001. Source of Support: Nil Code Number: is03053 ABSTRACT A patient with gross hydronephrosis presented with abdominal pain, vomiting, constipation and jaundice. Examination revealed features of tense ascites which when subjected to paracentesis revealed clear fluid. Further evaluation with imaging modalities revealed gross hydronephrosis with a non- functioning left kidney. Haematological and renal parameters were normal. Surgical removal of the affected kidney led to complete recovery with no postoperative consequences. KEY WORDS: Giant hydronephrosis, Ascites, Paracentesis, Nephrectomy. How to cite this article: Perwez Y, Singh H, Gondal PK. Cystic replacement of kidney mimicking ascites. Indian J Surg 2003;65:275-6. INTRODUCTION Unilateral cystic lesions of kidney including hydronephrosis usually present with a painless mass in the abdomen with no or minimal vague discomfort. Often these are discovered during the course of clinical examination or ultrasonography undertaken for other reasons. Presentation with acute abdominal symptoms is an uncommon occurrence. Hydronephrosis large enough to mimic features of ascites, which necessitated paracentesis, is a rare presentation. CASE REPORT A 40-year-old man was hospitalised with complaints of abdominal pain, vomiting, constipation and progressive distension of the abdomen for seven days. He was a chronic alcoholic and had jaundice on admission. Examination revealed a tense, distended and tender abdomen with presence of a fluid thrill. He was subjected to repeated paracentesis which revealed clear fluid which was transudative in nature. Routine haematological and renal parameters were within normal limits. Serum amylase was 225 IU/L, serum bilirubin 4.02 mg/dl, ALT-16 IU, ALP-74 IU. Plain X-ray abdomen gave a homogenous appearance. Ultrasonography abdomen suggested the possibility of loculated tubercular collection with ectopic or aberrant kidney or a gross hydronephrosis. CECT (contrast enhanced computerised tomography) abdomen showed huge cystic replacement of left kidney (Figure1). On nuclear scanning, left kidney was found non-functioning while the right one was normal. Exploration via a transverse incision and removal of a hugely cystic left kidney containing approximately 8 litres of urine showed histological features of xanthogranulomatous pyelonephritis. The ureter was normal. The patient had an uneventful postoperative period and was discharged on the 10th postoperative day. DISCUSSION Gross hydronephrosis large enough to mimic ascites is a rare presentation. This is also termed as giant hydronephrosis and around 200 cases have been reported so far. The diagnostic criteria include the presence of more than 1 litre of urine, radiologically, a mass occupying half of the abdomen or crossing the midline and with a height extending 5 vertebral bodies.1 Huge intraabdominal swelling is always a diagnostic dilemma, giant hydronephrosis being an unusual cause.2 The common differential diagnoses include ovarian cyst in females, pseudo-pancreatic cyst, mesenteric cyst and loculated peritoneal collection associated with tuberculosis or cirrhosis of the liver. Two cases of giant hydronephrosis mimicking ovarian cysts were reported associated with pregnancy.3 For giant hydronephrosis, nephrectomy is the treatment of choice.4 CONCLUSION Giant hydronephrosis is an unusual cause of huge intraabdominal swelling. It usually presents with vague clinical symptoms mimicking a variety of cystic lesions of the abdomen. A high degree of clinical suspicion is required to achieve the diagnosis. CECT of the abdomen is the best diagnostic modality available. Nephrectomy is the treatment of choice. ACKNOWLEDGEMENTS Our sincere thanks to Dr. M. N. Bhat, for critically analyzing the article and granting permission to publish the case report REFERENCES
Copyright 2003 - Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03053f1.jpg] |
| |||||||||

{kind=link}