 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 65, No. 3, May-June, 2003, pp. 279-280 Case Report Advanced metastatic prostate cancer presenting as a huge abdominal lump Iqbal Singh Department of Surgery, University College Of Medical Sciences (University of Delhi), and Guru Tegh Bahadur Hospital, Delhi 110095. India.
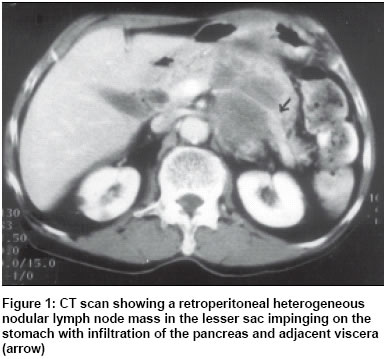
Paper Received: March 2002. Paper Accepted: July 2002. Source of Support: Nil Code Number: is03056 ABSTRACT An elderly male with severe cachexia and emaciation presented with a huge abdominal lump and a hard nodular prostate. Investigations revealed high stage metastatic adenocarcinoma of the prostate with a massive retroperitoneal hard, fixed nodular lymphnodal mass and a pancreatic mass. He was managed by total androgen blockade and orchidectomy. The literature regarding such malignancies has been reviewed and discussed. KEY WORDS: Prostate cancer, Metastases, Retroperitoneal lymph node. How to cite this article: Singh I. Advanced metastatic prostate cancer presenting as a huge abdominal lump. Indian J Surg 2003;65:279-80. INTRODUCTION Prostatic carcinomas generally spread to the bones of the spine and pelvis. The regional pelvic lymph nodes (obturator) are commonly involved. We report a rare and unusual type of advanced prostate adenocarcinoma in an elderly man with massive extra-regional lymph node and visceral metastasis presenting as huge abdominal mass at the time of initial presentation. He was detected to have a double metastatic advanced prostate adenocarcinoma involving the urinary bladder, pancreas and retroperitoneal lymph nodes. Orchidectomy and androgen ablation was partially effective. The literature regarding advanced cancer prostate with unusual presentations is reviewed and discussed herein. CASE REPORT An 86-year-old man presented with severe anaemia, cachexia, irritative voiding symptoms, gross total painless haematuria and a steadily increasing tender nodular fixed retroperitoneal upper abdominal lump (20 x 30 cm). Digital rectal examination revealed a hard nodule in the left lobe of prostate. Ultrasound and contrast enhanced computed tomography of the abdomen revealed a calcified lesion in the right antero-lateral bladder wall, a retroperitoneal nodular mass in the lesser sac impinging the lesser curvature of the stomach and infiltrating the body of the pancreas (Figure1). Urine cytology was positive for malignant epithelial cells and a trucut biopsy of the prostate confirmed a poorly differentiated prostate adenocarcinoma (Gleason score-8). Transurethral resection biopsy of the bladder tumour and aspiration biopsy of the abdominal lump revealed metastatic prostate adenocarcinoma. Chest X-ray and bone scan were negative while the serum prostate specific antigen (PSA) was 16 ng/ml. He was managed with a palliative transurethral resection of the bladder tumour (to control haematuria), androgen blockade with bilateral orchidectomy and oral flutamide 250 mg three times a day. Symptomatic improvement and partial reduction in the size of the mass were noticed after 3 months. He declined further treatment and was alive at a further follow-up of four months. DISCUSSION Though the adult male prostate does not contain any lymphatic vessel, carcinoma prostate most commonly metastasizes to regional lymph nodes1 and rarely metastasizes to the soft tissues.2 The spread of such cancers probably occurs through the rich peri-prostate lymphatic plexuses and is often preceded by capsular invasion. The regional lymph node disease is usually microscopic, asymptomatic and occurs more commonly in poorly differentiated prostate cancers. Extra-regional massive lymphadenopathy in carcinoma prostate as a presenting feature has not been reported in the surgical literature. Huge abdominal lumps due to massive retroperitoneal lymphadenopathy are rare in prostate cancers.2-5 These are usually poorly differentiated carcinomas with little or no rise in prostate specific antigen levels despite advanced bulky metastatic disease. Extensive local infiltration of the bladder neck and trigone area by a polypoidal secondary tumour leading to haematuria and positive urine cytology as happened in our case, possibly also occurs in such a subset of patients. Though patients with prostate cancer and PSA less than normal or in the lower range are not unusual (6-10%), it was the presence of three separate unusual metastatic sites from a locally advanced prostate cancer, which was intriguing, and uncommon. Rarely does adenocarcinoma of prostate present with such a large palpable abdominal mass3. It was also unusual that there were no bony metastasis in spite of such a massive tumour burden. Though orchidectomy is the standard treatment, contrary to previous reports,2,3 hormonal manipulation does not always result in a favourable response. The degree of differentiation may be a good prognostic indicator in this regard. Atypical presentation, positive urine cytology, calcification and sub-optimal response to hormonal manipulation, as in our case, represent prostate cancers with a different biological behaviour. However, no large experience exists in literature in treating such cases. Such cases probably represent unusual hurricane-like variants of androgen-insensitive giant metastatic prostate adenocarcinomas. We reported this case to alert the surgeon about the rare and bizarre manner in which prostate cancers may sometimes present, as a huge abdominal mass due to retroperitoneal lymphadenopathy. Prostate cancer should be included in the differential diagnosis of metastatic causes of large abdominal or retroperitoneal masses. Besides prostatic adenocarcinoma other rare prostate cancers should also be ruled out such as prostatic sarcomas, lymphomas, carcinosarcomas, chondro-sarcomas and squamous cell carcinoma of the prostate. REFERENCES
Copyright 2003 - Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03056f1.jpg] |
| |||||||||

{kind=link}